
FOOD & HEALTH SKEPTIC ARCHIVE
Monitoring food and health news
-- with particular attention to fads, fallacies and the "obesity" war
-- with particular attention to fads, fallacies and the "obesity" war
|
|
FOOD & HEALTH SKEPTIC ARCHIVE
Monitoring food and health news -- with particular attention to fads, fallacies and the "obesity" war |
The original version of this blog is HERE. Dissecting Leftism is HERE (and mirrored here). The Blogroll. My Home Page. Email me (John Ray) here. Other mirror sites: Greenie Watch, Political Correctness Watch, Education Watch, Recipes, Gun Watch, Australian Politics, Tongue Tied, Immigration Watch and Socialized Medicine. For a list of backups viewable in China, see here. The archives for this site are here or here. (Click "Refresh" on your browser if background colour is missing)
A major cause of increasing obesity is certainly the campaign against it -- as dieting usually makes people FATTER. If there were any sincerity to the obesity warriors, they would ban all diet advertising and otherwise shut up about it. Re-authorizing now-banned school playground activities and school outings would help too. But it is so much easier to blame obesity on the evil "multinationals" than it is to blame it on your own restrictions on the natural activities of kids
NOTE: "No trial has ever demonstrated benefits from reducing dietary saturated fat".
A brief summary of the last 50 years' of research into diet: Everything you can possibly eat or drink is both bad and good for you
****************************************************************************************
31 March, 2008
SUGAR CAUSES CANCER?
The post below is an excerpt from Sandy Szwarc. I myself made a derisive comment on the study that Sandy debunks on 11th. Sandy has however taken the trouble of looking at the study closely -- and finds that it is an even bigger fraud than I suspected. So this is yet another instance of the failure of peer-review in the madhouse that is the medical literature.
I see that Sandy has a critique coming up of the study about pot bellies that I dismissed on 28th. as "utter crap". Should be fun to see what she says! H/T to Ecomyths for drawing my attention to the article below. I should read Sandy regularly.
This new study was reported by the media as having found “conclusive evidence” that eating sugary cereals, white bread and other carbohydrates with high glycemic index increase risks of cancer and other modern “lifestyle diseases.”
This paper, published in the American Journal of Clinical Nutrition, was a meta-analysis of 37 published observational (epidemiological) studies that had looked for correlations between glycemic index/load and diseases. No cohort or clinical intervention trials were included.
The studies that the Australian authors compiled had differing designs: different age subjects; different study durations; different techniques to identify diseases (self-reported, chart reviews and only 4 involved actual physical exams); and had adjusted for different confounding factors known to contribute to disease. “Most of the studies used basic models, controlling for age and sex only,” however, the authors admitted.The studies used a food frequency questionnaire at enrollment to calculate GI/GL, but all used different units to report levels, so the authors converted the results to a single scale.
The authors noted that a significant limitation of their meta-analysis was that none of the studies they included had “actually validated the assessment of GI or GL using another dietary method or against an objective standard. The assignment of GI values to foods in a nutrient database is to some extent subjective,” they wrote, “and may be unreliable when extrapolating from one country to another.” They then separated out ten different diseases (type 2 diabetes, heart disease, stroke, breast cancer, colorectal cancer, pancreatic cancer, endometrial cancer, ovarian cancer, gastric cancer and gallbladder disease) and compiled the different risk ratios associated with GI/GL reported in each study.
This paper epitomized the weaknesses of meta-analyses, which lump together diverse and weak or null studies hoping to derive a significant effect. These problems make it imperative that any correlations that emerge from such analyses are tenable and clear; and beyond random chance, statistical modeling errors and confounding factors.
To cut to the chase, try as they might, they were unable to find a viable correlation between GI/GL and any disease. None of the 37 studies, separately or lumped together, could come up with a tenable link. The relative risks for all of the diseases hugged either side of null (relative risk 1/1 = 1):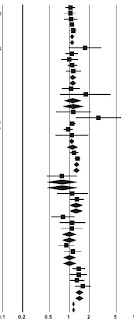
The researchers, however, arrived at a different conclusion:"This meta-analysis provides high-level evidence that diets with a high GI, high GL, or both, independently of known confounders, including fiber intake, increase the risk of chronic lifestyle-related diseases. The effect was modest overall... Overall, the GI had a more powerful effect than did the GL... The findings indicate that the judicious choice of low-GI foods offers a similar or higher level of protection as whole-grain foods or high fiber intake in the prevention of chronic lifestyle-related disease"Are we being sold something? When a study’s conclusions contrast so dramatically with the actual data, it is helpful to ask why.Not mentioned by any news reporter was that, except for the statisticians, the researchers who conducted this study are authors of GI diet books. Not only that, but they are with a GI testing service and a GI-based licensing program in Australia. Through the GI Symbol Program run out of the University of Sydney, food companies purchase license agreements with Glycemic Index Ltd. to put its GI symbol on their products. It’s a marketing gimmick, a “seal of approval” to identify foods for shoppers that are the “healthier choices.” The study’s lead author, Alan Barclay, is the founding director of GI Ltd., the company behind Australia’s GI Symbol Program, which is under the direction of another of the study authors, Jennie Brand-Miller....
With so much money and careers at stake in finding evidence to support low-GI foods, and in worrying people that high-GI foods could cause diseases and health problems, it might help explain why this study’s null findings were interpreted positively. Even the confirmation bias of well-meaning professionals can lead them to see proof of what they believe when the evidence disproves it.It’s not science itself that we can’t trust, it’s the bad portrayals of science.
Seeing for ourselves the actual null and negative findings, as was evident in all 37 studies on nearly 2 million people used in this analysis, offers us the most valuable information. If a significant correlation had been found and had biological plausability, a possible cause might then be tested by conducting randomized, controlled intervention clinical trials. If an epidemiological study can find no significant correlation, no link, between a food or ingredient and a disease, then there is nothing to base a suggestion for a causal link. It's a nonissue.
Null findings testing an hypothesis are important, as they enable science, and us, to move on, rather than continue to beat a dead horse or needlessly worry. This is the source of Albert Einstein’s famous saying: “No amount of experimentation can ever prove me right; a single experiment can prove me wrong.”
Study #2: No support for sugar fears
The second study was of no interest to PR agencies, and hence, never made the news. This epidemiological study, was published in the International Journal of Cancer. Its data was from 120,852 people in the Netherlands Cohort Study, who’d also completed food frequency questionnaires in 1986. After 11.3 years of follow-up, the researchers found no genuine relative risk for colorectal cancers related to dietary glycemic index or glycemic load among the men or women. They also found no clear associations between any cancer subsite and dietary factors. Relative risks for cancers associated with sugary, high-glycemic foods ranged from 0.83 to 1.20. The relative risks all hugged either side of null (RR=1) with none tenable, like the other observational studies.
Unlike the previous study, however, these researchers reported their findings factually: “Overall, our findings do not support the hypothesis that a diet with a high glycemic load or index is associated with a higher risk of colorectal cancer.” And conversely, low-glycemic foods aren’t associated with lower risks. There is no link. As hard as some have tried to prove that their believed way of eating is the only right way and can lead us all to optimum health and wellness, while preventing cancer and chronic diseases of aging; the facts continue to show that well-fed people around the world have hugely varied diets with no consistent correlations with health or longevity. More important, efforts to scare us about foods some don’t believe we should be eating and to prove that ‘bad’ foods can give us cancer or some other frightening disease have no credible evidence, either.
30 March, 2008
Happily Married Men and Women Have Lower Blood Pressure, Other Health Benefits
Happy people generally probably do
A report on research conducted at Brigham Young University reveals that men and women in happy marriages have substantially lower blood pressure than single individuals or couples in unhappy relationships.
Psychology professor Julianne Holt-Lunstad found that men and women in happy marriages scored four points lower than single adults during the course of a 24-hour blood pressure monitoring procedure. 204 married and 99 single adults were asked to wear unobtrusive portable blood pressure monitors which recorded blood pressure at random intervals throughout the day, even while participants slept. Each participant's blood pressure level was recorded about 72 times.
"There seem to be some unique health benefits from marriage," said Holt-Lunstad in a Science Daily report. "It's not just being married that benefits health - what's really the most protective of health is having a happy marriage." Not unexpectedly, the study found that unhappily married adults have higher blood pressure than both happily married and single adults.
LifeSiteNews.com has published many reports on the benefits to health and well-being of faithful marriage between one man and one woman, and the shortcomings of other types of relationships.
Dr. John Gottman, Professor of Psychology at the University of Washington in Seattle, who is well known for his research in the field of marriage, said, "The benefits (of faithful marriage) are better physical health, more resistance to infection, fewer infections, and a reduced likelihood of dying from cancer, from heart disease, from all major killers. The other health benefit is longevity: People live longer if they are in marital relationships, particularly if they are in good, satisfying relationships."
"There are physical benefits and mental health benefits," said Dr. Gottman. "You have less depression, less anxiety disorders, less psychosis, less posttraumatic stress disorders, fewer phobias. You also have fewer injuries due to accidents." He further states that "married men and women have lower suicide rates than unmarried ones because married people have meaningful social networks of friends and relatives. Meaningful relationships give people a sense of personal value and a feeling of responsibility to others." "Married individuals also tend to have stronger immune systems, making them less likely to catch colds and develop other illnesses than unmarried ones and that married persons are more likely to report feeling hopeful, happy, and good about themselves."
An interesting addendum to the research into the benefits of happily married couples is the statistics which show that perseverance in an unhappy marriage has a very decided benefit. The latest data show that within five years, just 12 percent of very unhappily married couples who stick it out are still unhappy; 70 percent of the formerly unhappiest couples now describe their marriage as "very" or "quite" happy.
Maggie Gallagher of the Manhattan Institute said, "Because marriage is a partnership in the whole of life, backed up by family, community, and religious values, marriage can do what economic partnerships don't: give a greater sense of meaning and purpose to life (a reason to exercise or cut back on booze, work harder, and to keep plugging even in the middle of those times when the marriage may not feel gratifying at all).
Married people are both responsible for and responsible to another human being, and both halves of that dynamic lead the married to live more responsible, fruitful, and satisfying lives. Marriage is a transformative act, changing the way two people look at each other, at the future, and at their roles in society. And it changes the way significant others - from family to congregation to insurance companies and the IRS - look at and treat that same couple. Sexual fidelity, an economic union, a parenting alliance, the promise of care that transcends day-to-day emotions: all these are what give a few words mumbled before a clergyman or judge the power to change lives."
Source
Smell compatibility
What makes us fall in love? Is it lust, mutual interests, shared life goals, or something much more intangible? Recent research suggests the latter. Researchers have only recently discovered an olfactory nerve that they believe is the route through which pheromones are processed. Nerve "O," as it is called, slipped under the radar for many years because it is so tiny. However, when the nerve was discovered in a whale, scientists surmised that this little nerve might be found in humans as well. And it was!
So what is the role of Nerve "O"? Nerve "O" has endings in the nasal cavity, but the fibers go directly to the sexual regions of the brain. Indeed, these endings entirely bypass the olfactory cortex! Hence we know the role of Nerve "O" is not to consciously smell, but to identify sexual cues from our potential partners.
What sexual cues do our scents give off? For one thing, we are more likely to be attracted to people whose scent is dissimilar to our own. Family members often share similar chemicals, so our attraction to differing chemical makeup suggests that sexual cues evolved to protect close family members from procreating together. On the other hand, pregnant women have been shown to be more drawn to people with similar chemical makeup, which might be due to the fact that during this crucial time, women are more apt to seek out family members than potential mates.
Research has also shown that these unconscious cues processed in Nerve "O" can make or break a relationship. Couples who have high levels of chemicals in common are more likely to encounter fertility issues, miscarriage and infidelity. The more dissimilar your and your partner's chemical makeup, the better chance you will have at successfully procreating and staying together.
So how can you create the scent that will keep you and your partner in the land of happily ever after? Unfortunately, you can't. Perfumes and colognes can't fool Nerve "O" - the scents that humans and animals are attracted to are intangible and instinctive. Even the most expensive designer perfume can't fool Mother Nature. When it comes to sexual attraction, it seems you really have to leave things in the air!
However, if you are taking a hormonal contraceptive, you might be bucking an evolutionary tide. Women who are on the pill are more likely to be attracted to men with similar chemical makeup - most likely because their bodies are fooling them into believing they are pregnant, and so much like actual pregnant women, their Nerve "O" leads them to kin and not mates. So if you were on the pill when you met your mate, you might experience a diminishing attraction when you cease taking it. Only time will tell what role Nerve "O" plays in future sex research, but one thing is for sure: When it comes to true love, follow your nose!
Source
****************
Just some problems with the "Obesity" war:
1). It tries to impose behavior change on everybody -- when most of those targeted are not obese and hence have no reason to change their behaviour. It is a form of punishing the innocent and the guilty alike. (It is also typical of Leftist thinking: Scorning the individual and capable of dealing with large groups only).
2). The longevity research all leads to the conclusion that it is people of MIDDLING weight who live longest -- not slim people. So the "epidemic" of obesity is in fact largely an "epidemic" of living longer.
3). It is total calorie intake that makes you fat -- not where you get your calories. Policies that attack only the source of the calories (e.g. "junk food") without addressing total calorie intake are hence pissing into the wind. People involuntarily deprived of their preferred calorie intake from one source are highly likely to seek and find their calories elsewhere.
4). So-called junk food is perfectly nutritious. A big Mac meal comprises meat, bread, salad and potatoes -- which is a mainstream Western diet. If that is bad then we are all in big trouble.
5). Food warriors demonize salt and fat. But we need a daily salt intake to counter salt-loss through perspiration and the research shows that people on salt-restricted diets die SOONER. And Eskimos eat huge amounts of fat with no apparent ill-effects. And the average home-cooked roast dinner has LOTS of fat. Will we ban roast dinners?
6). The foods restricted are often no more calorific than those permitted -- such as milk and fruit-juice drinks.
7). Tendency to weight is mostly genetic and is therefore not readily susceptible to voluntary behaviour change.
8). And when are we going to ban cheese? Cheese is a concentrated calorie bomb and has lots of that wicked animal fat in it too. Wouldn't we all be better off without it? And what about butter and margarine? They are just about pure fat. Surely they should be treated as contraband in kids' lunchboxes! [/sarcasm].
9). And how odd it is that we never hear of the huge American study which showed that women who eat lots of veggies have an INCREASED risk of stomach cancer? So the official recommendation to eat five lots of veggies every day might just be creating lots of cancer for the future! It's as plausible (i.e. not very) as all the other dietary "wisdom" we read about fat etc.
10). And will "this generation of Western children be the first in history to lead shorter lives than their parents did"? This is another anti-fat scare that emanates from a much-cited editorial in a prominent medical journal that said so. Yet this editorial offered no statistical basis for its opinion -- an opinion that flies directly in the face of the available evidence.
Even statistical correlations far stronger than anything found in medical research may disappear if more data is used. A remarkable example from Sociology:"The modern literature on hate crimes began with a remarkable 1933 book by Arthur Raper titled The Tragedy of Lynching. Raper assembled data on the number of lynchings each year in the South and on the price of an acre's yield of cotton. He calculated the correlation coefficient between the two series at -0.532. In other words, when the economy was doing well, the number of lynchings was lower.... In 2001, Donald Green, Laurence McFalls, and Jennifer Smith published a paper that demolished the alleged connection between economic conditions and lynchings in Raper's data. Raper had the misfortune of stopping his analysis in 1929. After the Great Depression hit, the price of cotton plummeted and economic conditions deteriorated, yet lynchings continued to fall. The correlation disappeared altogether when more years of data were added."So we must be sure to base our conclusions on ALL the data. But in medical research, data selectivity and the "overlooking" of discordant research findings is epidemic.
"What we should be doing is monitoring children from birth so we can detect any deviations from the norm at an early stage and action can be taken". Who said that? Joe Stalin? Adolf Hitler? Orwell's "Big Brother"? The Spanish Inquisition? Generalissimo Francisco Franco Bahamonde? None of those. It was Dr Colin Waine, chairman of Britain's National Obesity Forum. What a fine fellow!
*********************
29 March, 2008
Coronary Calcification Predicts Future Heart Attacks and Coronary Death. Cholesterol Not Found To Be A Significant Risk Factor
A striking report just published in the New England Journal of Medicine indicates the accumulation of calcium in coronary arteries, and not cholesterol, more accurately predicts a future heart attack or other heart trouble, far more than cholesterol or other standard risk factors.
This report gives evidence of a major misdirection by modern medicine - the creation of cholesterol phobia in the population at large. Prior studies show use of cholesterol-lowering drugs does not reduce mortality rates for coronary artery disease. This report follows a front-page report in Business Week Magazine declaring cholesterol-lowering drugs to be of marginal value.
The study involved 6722 men and women, ~age 60, who were studied for a period of 3.8 years (median). None had coronary artery disease at the beginning of the study. Subjects who experienced an adverse coronary event (heart attack, angina, placement of a stent, coronary death) were more likely to be taking cholesterol-lowering drugs (~28%) than those who did not experience such an event (~16%). Furthermore, subjects who experienced a heart attack or angina had about the same total cholesterol (~199) as subjects who did not (~194). Cholesterol barely met statistical significance whereas calcium was a highly predictive factor.
Traditionally-used risk factors, such as C-reactive protein (a marker of inflammation), triglycerides, HDL cholesterol and greater body mass, were not predictive for a future coronary artery event.
Among subjects whose coronary artery calcium score was zero, their risk for any adverse coronary event was only about one-half of 1% (0.0044), or less than 1 in 200, whereas those with a coronary calcium score over 300, about 8.0% experienced an adverse event involving coronary arteries (0.0804), or about 8 in 100, an 18-fold difference (1800%!), over the 3.8 year period.
This study shows the risk for a future heart attack is nil for those with a calcium arterial score of zero. This data helps to explain why hundreds of thousands of Americans experience a sudden-death heart attack with low-to-normal cholesterol. Most heart attacks emanate in the four coronary arteries that supply the heart with oxygenated blood. About 50% of arterial plaque is calcium and only 3% is cholesterol.
Arterial calcium can be measured by use of a CT scan (called an Agatston score, for Dr. Arthur Agatston, South Beach Miami, Florida cardiologist). About 70% of white males, 52% of black males, 57% of Hispanic males and 59% of Chinese males, have coronary calcium scores greater than zero. The calcium arterial scores for women are about half that of males owing to the fact they donate calcium to their offspring during pregnancy and lactation and control calcium via estrogen throughout their fertile years.
Calcium begins to accumulate in coronary arteries in males as soon as full growth is achieved, around age 18. Women begin to accumulate calcium in their arteries with the onset of menopause or early hysterectomy. It was recently reported that postmenopausal women who take calcium supplements increase their risk for a heart attack by about 45%. [British Medical Journal 2008 Feb 2; 336 (7638): 262-6]
In the early 1990s British cardiologist Stephen Seely noted that countries which consume that highest amount of calcium (New Zealand, Ireland, North America, Scandinavian countries), mostly from dairy products, have the highest rates of cardiovascular disease. [International Journal Cardiology 1991 Nov; 33(2):191-8]
Sixty-four percent (64%) of subjects who experienced any coronary event were current or former smokers compared to about 50% of those who did not experience a heart attack or other adverse event.
Source
(See Coronary Calcium as a Predictor of Coronary Events in Four Racial or Ethnic Groups, New England Journal of Medicine 358: 1336-45, March 27, 2008)
Laboratory evidence shows red wine antioxidant kills cancer
Are we allowed to mention that antioxidants shorten your lifespan?
Rochester researchers showed for the first time that a natural antioxidant found in grape skins and red wine can help destroy pancreatic cancer cells by reaching to the cell's core energy source, or mitochondria, and crippling its function. The study is published in the March edition of the journal, Advances in Experimental Medicine and Biology. The study also showed that when the pancreatic cancer cells were doubly assaulted -- pre-treated with the antioxidant, resveratrol, and irradiated -- the combination induced a type of cell death called apoptosis, an important goal of cancer therapy.
The research has many implications for patients, said lead author Paul Okunieff, M.D., chief of Radiation Oncology at the James P. Wilmot Cancer Center at the University of Rochester Medical Center.
Although red wine consumption during chemotherapy or radiation treatment has not been well studied, it is not "contraindicated," Okunieff said. In other words, if a patient already drinks red wine moderately, most physicians would not tell the patient to give it up during treatment. Perhaps a better choice, Okunieff said, would be to drink as much red or purple grape juice as desired.
Yet despite widespread interest in antioxidants, some physicians are concerned antioxidants might end up protecting tumors. Okunieff's study showed there is little evidence to support that fear. In fact, the research suggests resveratrol not only reaches its intended target, injuring the nexus of malignant cells, but at the same time protects normal tissue from the harmful effects of radiation.
"Antioxidant research is very active and very seductive right now," Okunieff said. "The challenge lies in finding the right concentration and how it works inside the cell. In this case, we've discovered an important part of that equation. Resveratrol seems to have a therapeutic gain by making tumor cells more sensitive to radiation and making normal tissue less sensitive."
Resveratrol is known for its ability to protect plants from bacteria and fungi. Purified versions have been described in scientific journals as potential anti-cancer, anti-inflammatory and anti-atherogenic agents, and for their ability to modulate cell growth. Other well-known antioxidants derived from natural sources include caffeine, melatonin, flavonoids, polyphenols, and vitamins C and E.
A flurry of antioxidant studies in recent years has not proven how and why they work at the cellular level. At the suggestion of a young scientist in his lab, Okunieff began studying resveratrol as a tumor sensitizer. That's when they discovered its link to the mitochondria. The discovery is critical because, like the cell nucleus, the mitochondria contains its own DNA and has the ability to continuously supply the cell with energy when functioning properly. Stopping the energy flow theoretically stops the cancer.
Researchers divided pancreatic cancer cells into two groups: cells treated without resveratrol, or with resveratrol, at a relatively high dose of 50 mg/ml, in combination with ionizing radiation. (The resveratrol concentration in red wine can be as high as 30 mg/ml, the study said, and higher doses are expected to be safe as long as a physician is monitoring.)
They evaluated the mitochondria function of the cells treated with resveratrol, and also measured apoptosis (cell death), the level of reactive oxygen species in the cells, and how the cell membranes responded to the antioxidant.
Laboratory experiments showed that resveratrol:
-- Reduced the function of proteins in the pancreatic cancer cell membranes that are responsible for pumping chemotherapy out of the cell, making the cells chemo-sensitive.
-- Triggered the production of reactive oxygen species (ROS), which are substances circulating in the human body that have been implicated in a number of diseases: when ROS is increased, cells burn out and die.
-- Caused apoptosis, which is likely the result of increased ROS.
-- Depolarized the mitochondrial membranes, which indicates a decrease in the cell's potential to function. Radiation alone does not injure the mitochondrial membrane as much.
The team also wanted to investigate why pancreatic cancer cells seem to be particularly resistant to chemotherapy. The pancreas, a gland located deep in the abdomen, produces insulin and regulates sugar, and pumps or channels powerful digestive enzymes into the duodenum. This natural pumping process, however, ends up ridding the needed chemotherapy from cells in the pancreas. But just as reseveratrol interferes with the cancer cells' energy source, it also may decrease the power available to pump chemotherapy out of the cell.
"While additional studies are needed," Okunieff said, "this research indicates that resveratrol has a promising future as part of the treatment for cancer."
In the same journal, Okunieff and his group also reviewed why resveratrol protects normal tissue, and found that antioxidants can be designed to take advantage of certain biochemical properties or cellular targets, making them more effective.
Source
****************
Just some problems with the "Obesity" war:
1). It tries to impose behavior change on everybody -- when most of those targeted are not obese and hence have no reason to change their behaviour. It is a form of punishing the innocent and the guilty alike. (It is also typical of Leftist thinking: Scorning the individual and capable of dealing with large groups only).
2). The longevity research all leads to the conclusion that it is people of MIDDLING weight who live longest -- not slim people. So the "epidemic" of obesity is in fact largely an "epidemic" of living longer.
3). It is total calorie intake that makes you fat -- not where you get your calories. Policies that attack only the source of the calories (e.g. "junk food") without addressing total calorie intake are hence pissing into the wind. People involuntarily deprived of their preferred calorie intake from one source are highly likely to seek and find their calories elsewhere.
4). So-called junk food is perfectly nutritious. A big Mac meal comprises meat, bread, salad and potatoes -- which is a mainstream Western diet. If that is bad then we are all in big trouble.
5). Food warriors demonize salt and fat. But we need a daily salt intake to counter salt-loss through perspiration and the research shows that people on salt-restricted diets die SOONER. And Eskimos eat huge amounts of fat with no apparent ill-effects. And the average home-cooked roast dinner has LOTS of fat. Will we ban roast dinners?
6). The foods restricted are often no more calorific than those permitted -- such as milk and fruit-juice drinks.
7). Tendency to weight is mostly genetic and is therefore not readily susceptible to voluntary behaviour change.
8). And when are we going to ban cheese? Cheese is a concentrated calorie bomb and has lots of that wicked animal fat in it too. Wouldn't we all be better off without it? And what about butter and margarine? They are just about pure fat. Surely they should be treated as contraband in kids' lunchboxes! [/sarcasm].
9). And how odd it is that we never hear of the huge American study which showed that women who eat lots of veggies have an INCREASED risk of stomach cancer? So the official recommendation to eat five lots of veggies every day might just be creating lots of cancer for the future! It's as plausible (i.e. not very) as all the other dietary "wisdom" we read about fat etc.
10). And will "this generation of Western children be the first in history to lead shorter lives than their parents did"? This is another anti-fat scare that emanates from a much-cited editorial in a prominent medical journal that said so. Yet this editorial offered no statistical basis for its opinion -- an opinion that flies directly in the face of the available evidence.
Even statistical correlations far stronger than anything found in medical research may disappear if more data is used. A remarkable example from Sociology:"The modern literature on hate crimes began with a remarkable 1933 book by Arthur Raper titled The Tragedy of Lynching. Raper assembled data on the number of lynchings each year in the South and on the price of an acre's yield of cotton. He calculated the correlation coefficient between the two series at -0.532. In other words, when the economy was doing well, the number of lynchings was lower.... In 2001, Donald Green, Laurence McFalls, and Jennifer Smith published a paper that demolished the alleged connection between economic conditions and lynchings in Raper's data. Raper had the misfortune of stopping his analysis in 1929. After the Great Depression hit, the price of cotton plummeted and economic conditions deteriorated, yet lynchings continued to fall. The correlation disappeared altogether when more years of data were added."So we must be sure to base our conclusions on ALL the data. But in medical research, data selectivity and the "overlooking" of discordant research findings is epidemic.
"What we should be doing is monitoring children from birth so we can detect any deviations from the norm at an early stage and action can be taken". Who said that? Joe Stalin? Adolf Hitler? Orwell's "Big Brother"? The Spanish Inquisition? Generalissimo Francisco Franco Bahamonde? None of those. It was Dr Colin Waine, chairman of Britain's National Obesity Forum. What a fine fellow!
*********************
28 March, 2008
Pot bellies linked to dementia
This is utter crap. It is another outing for the fallacy, much-loved in medical medical research, that correlation is causation. It shows that there is a slight tendency for the small minority of people who get Alzheimer's to have bigger bellies in mid-life. But to say that the big bellies CAUSE Alzheimer's is pure speculation. Given the lack of any obvious connection between the two phenomena, it is much more likely that whatever it is that brings on Alzheimers also has the side effect of increasing abdominal fat. And note that the study was done in Northern California, where half the population seems to be stoned out of their brains for much of the time. Perhaps the bad stuff that they pump into themselves both makes them fat and blasts their brains
Having a large belly in middle age nearly triples the risk of developing dementia, a study released today found. Being overweight in midlife and beyond has long been linked to increased risk for disease such as stroke, diabetes and heart disease. But this is the first study to link excess fat to dementia and, the research found excess abdominal fat increased the risk even among those who were of normal weight overall.
"Considering that 50 per cent of adults in this country (US) have abdominal obesity, this is a disturbing finding," said study author Rachel Whitmer of the Kaiser Permanente Division of Research in Oakland, California.
Researchers measured the abdominal fat of 6583 people age 40 to 45 in northern California and some 36 years later 16 per cent had developed dementia, the study published in the journal Neurology found. Those who were overweight or obese but did not have a pot belly had an 80 per cent increase in the risk of dementia compared to people with a normal body weight and abdominal fat level. The risk increase jumped to 230 per cent among overweight people with a large belly and 360 per cent among the obese with large abdomens. "Where one carries the weight - especially in midlife - appears to be an important predictor for dementia risk," Ms Whitmer said.
While more research is needed to understand why this link exists, it is possible that the abdominal obesity is part of a complex set of health-related behaviours that increase the risk of dementia. "Autopsies have shown that changes in the brain associated with Alzheimer's disease may start in young to middle adulthood, and another study showed that high abdominal fat in elderly adults was tied to greater brain atrophy," she said. "These findings imply that the dangerous effects of abdominal obesity on the brain may start long before the signs of dementia appear."
Source
"Bootcamp" for fat kids?
This is REALLY getting Fascist
Bootcamp in schools is not necessary and teachers should not cop the blame for unfit children, the State Government said yesterday. Education Minister David Bartlett said schools were already doing enough to ensure kids were fit and healthy and parents needed to play a larger role. He said bootcamp was "too extreme", school curriculums were already crowded, and schools needed to focus on literacy and numeracy over sport.
His comments come after high-profile TV fitness trainer Michelle Bridges, from the TV show The Biggest Loser, said Tasmanian students should undertake high-intensity bootcamp for at least 30 minutes at the start of each school day to reduce skyrocketing obesity rates. Bridges said she was shocked Tasmania had one of the nation's highest obesity rates and that doctors had been treating children as young as two for obesity-related health conditions. And she said Tasmanian schools could lead the nation with daily bootcamps which would have "massive results" on students' exercise, nutrition and learning.
But Mr Bartlett said he did not support bootcamps and was confident students already did enough exercise at school. "I don't like the term bootcamp because it's too extreme," Mr Bartlett said. "But in fact there are physical education programs happening in all our schools, and some of the best ones are those style of things where kids get out in the morning, do their exercise, get ready and come back in and start learning. "We have mandated two hours of physical education a week in every school in Tasmania, and in almost every school I've been into physical activity and education happens every day."
He said parents needed to stop blaming schools for unfit children, and do more at home to encourage exercise and good eating habits. "It's a crowded curriculum and people in Tasmania, I believe, as my number one priority, want me to lift literacy and numeracy rates and that's what we're working hard on," Mr Bartlett said. He said more emphasis needed to be put on what happened at home.
Source
****************
Just some problems with the "Obesity" war:
1). It tries to impose behavior change on everybody -- when most of those targeted are not obese and hence have no reason to change their behaviour. It is a form of punishing the innocent and the guilty alike. (It is also typical of Leftist thinking: Scorning the individual and capable of dealing with large groups only).
2). The longevity research all leads to the conclusion that it is people of MIDDLING weight who live longest -- not slim people. So the "epidemic" of obesity is in fact largely an "epidemic" of living longer.
3). It is total calorie intake that makes you fat -- not where you get your calories. Policies that attack only the source of the calories (e.g. "junk food") without addressing total calorie intake are hence pissing into the wind. People involuntarily deprived of their preferred calorie intake from one source are highly likely to seek and find their calories elsewhere.
4). So-called junk food is perfectly nutritious. A big Mac meal comprises meat, bread, salad and potatoes -- which is a mainstream Western diet. If that is bad then we are all in big trouble.
5). Food warriors demonize salt and fat. But we need a daily salt intake to counter salt-loss through perspiration and the research shows that people on salt-restricted diets die SOONER. And Eskimos eat huge amounts of fat with no apparent ill-effects. And the average home-cooked roast dinner has LOTS of fat. Will we ban roast dinners?
6). The foods restricted are often no more calorific than those permitted -- such as milk and fruit-juice drinks.
7). Tendency to weight is mostly genetic and is therefore not readily susceptible to voluntary behaviour change.
8). And when are we going to ban cheese? Cheese is a concentrated calorie bomb and has lots of that wicked animal fat in it too. Wouldn't we all be better off without it? And what about butter and margarine? They are just about pure fat. Surely they should be treated as contraband in kids' lunchboxes! [/sarcasm].
9). And how odd it is that we never hear of the huge American study which showed that women who eat lots of veggies have an INCREASED risk of stomach cancer? So the official recommendation to eat five lots of veggies every day might just be creating lots of cancer for the future! It's as plausible (i.e. not very) as all the other dietary "wisdom" we read about fat etc.
10). And will "this generation of Western children be the first in history to lead shorter lives than their parents did"? This is another anti-fat scare that emanates from a much-cited editorial in a prominent medical journal that said so. Yet this editorial offered no statistical basis for its opinion -- an opinion that flies directly in the face of the available evidence.
Even statistical correlations far stronger than anything found in medical research may disappear if more data is used. A remarkable example from Sociology:"The modern literature on hate crimes began with a remarkable 1933 book by Arthur Raper titled The Tragedy of Lynching. Raper assembled data on the number of lynchings each year in the South and on the price of an acre's yield of cotton. He calculated the correlation coefficient between the two series at -0.532. In other words, when the economy was doing well, the number of lynchings was lower.... In 2001, Donald Green, Laurence McFalls, and Jennifer Smith published a paper that demolished the alleged connection between economic conditions and lynchings in Raper's data. Raper had the misfortune of stopping his analysis in 1929. After the Great Depression hit, the price of cotton plummeted and economic conditions deteriorated, yet lynchings continued to fall. The correlation disappeared altogether when more years of data were added."So we must be sure to base our conclusions on ALL the data. But in medical research, data selectivity and the "overlooking" of discordant research findings is epidemic.
"What we should be doing is monitoring children from birth so we can detect any deviations from the norm at an early stage and action can be taken". Who said that? Joe Stalin? Adolf Hitler? Orwell's "Big Brother"? The Spanish Inquisition? Generalissimo Francisco Franco Bahamonde? None of those. It was Dr Colin Waine, chairman of Britain's National Obesity Forum. What a fine fellow!
*********************
27 March, 2008
Hairdressers face cancer risk?
This is really crazy. They admit that hairdressers smoke more so could that be the cause of the slightly higher rate of cancer? "Probably" not, we read. It's just speculation and it's not even good speculation. What chemicals do barbers get exposed to? A bit of antiseptic is all as far as I know. Female hairdressers on the other hand use LOTS of chemicals. So why is the risk high in men and low in women? If chemicals were the problem it would be the other way around. It's just amazing that this trash got published at all -- let alone in "Lancet". Lancet has gone far down hill from what it once was. In the context of its conversion to Green/Left thinking that is not surprising. Facts are a very low priority for the Left. Creating disruption is what they live for
Hairdressers may face an increased risk of cancer because of the dyes and other chemicals they work with, says the World Health Organisation's International Agency for Research on Cancer (IARC). "Occupation as a hairdresser or barber entails exposures that are probably carcinogenic," says a report compiled by a working group for the agency, which is based in Lyon, southern France.
The study is a review of half a dozen large investigations into cancer risk. Among male hairdressers and barbers, the risk of cancer of the bladder was between 20 and 60 per cent higher compared with the general population, the study says. The risk is described as "small but consistent" and is less visible among women.
Among both men and women, some studies pointed to a heightened risk of 30 per cent for lung cancer, although this could be partly explained by higher incidence of smoking among hairdressers. Among women alone, some studies pointed to an increased risk for ovarian cancer and of non-Hodgkin's lymphoma. The journal The Lancet Oncology reports on the study in its latest issue, out today.
Source
Diabetes remedy?

Bitter melon, an ancient Chinese remedy, contains a powerful treatment for Type 2 diabetes, Sydney-based researchers have found. A team from the Garvan Institute of Medical Research, along with the Shanghai Institute of Materia Medica, found that fruit known in South-East Asia as pare contains four bioactive compounds.
They all appear to activate the enzyme AMPK, a protein that regulates the body's metabolism and affects glucose uptake, according to research published yesterday in Chemistry and Biology. One of the compounds increased fatty acid oxidation and glucose disposal in the body, potentially helping tackle diabetes and obesity. "We can now understand at a molecular level why bitter melon works as a treatment for diabetes," David James, director of the diabetes and obesity program at Garvan said. "By isolating the compounds we believe to be therapeutic, we can investigate how they work together in our cells," Professor James said.
The researchers said other diabetes drugs already available also activated AMPK but they could have side-effects. "The advantage of bitter melon is that there are no known side-effects," said Dr Jiming Ye. "Practitioners of Chinese medicine have used it for hundreds of years to good effect." The fruit was described in a 16th century compendium of Chinese medicine as "expelling evil heat, relieving fatigue and illuminating". But previous studies have warned that children and pregnant women should not use bitter melon because of its potential toxicity.
Source
****************
Just some problems with the "Obesity" war:
1). It tries to impose behavior change on everybody -- when most of those targeted are not obese and hence have no reason to change their behaviour. It is a form of punishing the innocent and the guilty alike. (It is also typical of Leftist thinking: Scorning the individual and capable of dealing with large groups only).
2). The longevity research all leads to the conclusion that it is people of MIDDLING weight who live longest -- not slim people. So the "epidemic" of obesity is in fact largely an "epidemic" of living longer.
3). It is total calorie intake that makes you fat -- not where you get your calories. Policies that attack only the source of the calories (e.g. "junk food") without addressing total calorie intake are hence pissing into the wind. People involuntarily deprived of their preferred calorie intake from one source are highly likely to seek and find their calories elsewhere.
4). So-called junk food is perfectly nutritious. A big Mac meal comprises meat, bread, salad and potatoes -- which is a mainstream Western diet. If that is bad then we are all in big trouble.
5). Food warriors demonize salt and fat. But we need a daily salt intake to counter salt-loss through perspiration and the research shows that people on salt-restricted diets die SOONER. And Eskimos eat huge amounts of fat with no apparent ill-effects. And the average home-cooked roast dinner has LOTS of fat. Will we ban roast dinners?
6). The foods restricted are often no more calorific than those permitted -- such as milk and fruit-juice drinks.
7). Tendency to weight is mostly genetic and is therefore not readily susceptible to voluntary behaviour change.
8). And when are we going to ban cheese? Cheese is a concentrated calorie bomb and has lots of that wicked animal fat in it too. Wouldn't we all be better off without it? And what about butter and margarine? They are just about pure fat. Surely they should be treated as contraband in kids' lunchboxes! [/sarcasm].
9). And how odd it is that we never hear of the huge American study which showed that women who eat lots of veggies have an INCREASED risk of stomach cancer? So the official recommendation to eat five lots of veggies every day might just be creating lots of cancer for the future! It's as plausible (i.e. not very) as all the other dietary "wisdom" we read about fat etc.
10). And will "this generation of Western children be the first in history to lead shorter lives than their parents did"? This is another anti-fat scare that emanates from a much-cited editorial in a prominent medical journal that said so. Yet this editorial offered no statistical basis for its opinion -- an opinion that flies directly in the face of the available evidence.
Even statistical correlations far stronger than anything found in medical research may disappear if more data is used. A remarkable example from Sociology:"The modern literature on hate crimes began with a remarkable 1933 book by Arthur Raper titled The Tragedy of Lynching. Raper assembled data on the number of lynchings each year in the South and on the price of an acre's yield of cotton. He calculated the correlation coefficient between the two series at -0.532. In other words, when the economy was doing well, the number of lynchings was lower.... In 2001, Donald Green, Laurence McFalls, and Jennifer Smith published a paper that demolished the alleged connection between economic conditions and lynchings in Raper's data. Raper had the misfortune of stopping his analysis in 1929. After the Great Depression hit, the price of cotton plummeted and economic conditions deteriorated, yet lynchings continued to fall. The correlation disappeared altogether when more years of data were added."So we must be sure to base our conclusions on ALL the data. But in medical research, data selectivity and the "overlooking" of discordant research findings is epidemic.
"What we should be doing is monitoring children from birth so we can detect any deviations from the norm at an early stage and action can be taken". Who said that? Joe Stalin? Adolf Hitler? Orwell's "Big Brother"? The Spanish Inquisition? Generalissimo Francisco Franco Bahamonde? None of those. It was Dr Colin Waine, chairman of Britain's National Obesity Forum. What a fine fellow!
*********************
26 March, 2008
ANOTHER FISHY STORY
The old "wonders of fish" story again! Popular summary followed by journal abstract below. There is a lot of scorn that I could pour on this study (control for education and income etc.?) but I will content myself with noting that IQ at age 3 cannot reliably be assessed
Pregnant women who regularly eat fish can give their children a head start in life by boosting their intelligence, a study has found. The children of mothers who ate fish more than twice a week during their second trimester were better in language and motor skill tests, research at Harvard University found
But it also showed the effects may depend on the type of fish eaten. The study, which monitored more than 300 children at three stages of development, counters advice that pregnant women should avoid fish because it can contain toxic chemicals.
"Dietary recommendations for pregnant women should incorporate the nutritional benefits as well as the risks of fish intake," the report, which will be published in the American Journal of Epidemiology this week, concluded.
Source
Maternal Fish Intake during Pregnancy, Blood Mercury Levels, and Child Cognition at Age 3 Years in a US Cohort
By Emily Oken et al
The balance of contaminant risk and nutritional benefit from maternal prenatal fish consumption for child cognitive development is not known. Using data from a prospective cohort study of 341 mother-child pairs in Massachusetts enrolled in 1999-2002, the authors studied associations of maternal second-trimester fish intake and erythrocyte mercury levels with children's scores on the Peabody Picture Vocabulary Test (PPVT) and Wide Range Assessment of Visual Motor Abilities (WRAVMA) at age 3 years. Mean maternal total fish intake was 1.5 (standard deviation, 1.4) servings/month, and 40 (12%) mothers consumed >2 servings/week. Mean maternal mercury level was 3.8 (standard deviation, 3.8) ng/g. After adjustment using multivariable linear regression, higher fish intake was associated with better child cognitive test performance, and higher mercury levels with poorer test scores. Associations strengthened with inclusion of both fish and mercury: effect estimates for fish intake of >2 servings/week versus never were 2.2 (95% confidence interval (CI): -2.6, 7.0) for the PPVT and 6.4 (95% CI: 2.0, 10.8) for the WRAVMA; for mercury in the top decile, they were -4.5 (95% CI: -8.5, -0.4) for the PPVT and -4.6 (95% CI: -8.3, -0.9) for the WRAVMA. Fish consumption of ~2 servings/week was not associated with a benefit. Dietary recommendations for pregnant women should incorporate the nutritional benefits as well as the risks of fish intake.
Source
Breast cancer risk test on the way

GENETIC research is moving so fast that a Brisbane scientist believes a blood test may be available to calculate a woman's breast cancer risk within five years. Georgia Chenevix-Trench, of the Queensland Institute of Medical Research, is part of a global team of scientists involved in searching for breast cancer susceptibility genes. "What you could do is give women a risk assessment at different ages," she said. "That might be a reality within a few years."
Dr Chenevix-Trench said no test was likely to be able to tell women categorically whether they would develop breast cancer. Lifestyle factors and environment are also believed to play a role. But a blood test should be able to tell women whether they were at high or low risk - or somewhere in-between - at varying stages of their lives based on their genetic profile. "Maybe women who are lining up for mammograms would have a blood test and they would be told: 'You're at a very high risk, you should have additional screening'," Dr Chenevix-Trench said. "If you're at very low risk, you possibly could reduce your frequency. It's a political hot potato to suggest that some people could have less screening but I think you could probably do that."
Australian women have a one-in-eight chance of developing breast cancer in their lifetime. Scientists have known for years that defects in two genes, BRCA1 and BRCA2, give women a much higher risk of breast cancer. Some women found with defects in those genes opt for mastectomies and ovary removal to dramatically cut their odds of cancer.
A paper published recently in the American Journal of Human Genetics, co-written by Dr Chenevix-Trench, found variations in two genes, known as FGFR2 and TNRC9, amplified a woman's breast cancer risk if she also carried the BRCA2 defect. The research found BRCA2 defect carriers with the highest risk combination of FGFR2 and TNRC9 genes had a 70 per cent likelihood of developing breast cancer.
Source
Cod liver oil lubricates your bones! "A regular dose of cod liver oil reduces the quantity of painkilling drugs needed by people with rheumatoid arthritis (RA), a study in Scotland has found. The finding, published in Rheumatology magazine, is significant because cod liver oil is benign, whereas nonsteroidal antiinflammatory drugs, such as ibuprofen or naproxen, which are commonly taken by RA patients, can have serious side-effects. The study was carried out over five years by researchers from rheumatology units in Dundee and Edinburgh.
****************
Just some problems with the "Obesity" war:
1). It tries to impose behavior change on everybody -- when most of those targeted are not obese and hence have no reason to change their behaviour. It is a form of punishing the innocent and the guilty alike. (It is also typical of Leftist thinking: Scorning the individual and capable of dealing with large groups only).
2). The longevity research all leads to the conclusion that it is people of MIDDLING weight who live longest -- not slim people. So the "epidemic" of obesity is in fact largely an "epidemic" of living longer.
3). It is total calorie intake that makes you fat -- not where you get your calories. Policies that attack only the source of the calories (e.g. "junk food") without addressing total calorie intake are hence pissing into the wind. People involuntarily deprived of their preferred calorie intake from one source are highly likely to seek and find their calories elsewhere.
4). So-called junk food is perfectly nutritious. A big Mac meal comprises meat, bread, salad and potatoes -- which is a mainstream Western diet. If that is bad then we are all in big trouble.
5). Food warriors demonize salt and fat. But we need a daily salt intake to counter salt-loss through perspiration and the research shows that people on salt-restricted diets die SOONER. And Eskimos eat huge amounts of fat with no apparent ill-effects. And the average home-cooked roast dinner has LOTS of fat. Will we ban roast dinners?
6). The foods restricted are often no more calorific than those permitted -- such as milk and fruit-juice drinks.
7). Tendency to weight is mostly genetic and is therefore not readily susceptible to voluntary behaviour change.
8). And when are we going to ban cheese? Cheese is a concentrated calorie bomb and has lots of that wicked animal fat in it too. Wouldn't we all be better off without it? And what about butter and margarine? They are just about pure fat. Surely they should be treated as contraband in kids' lunchboxes! [/sarcasm].
9). And how odd it is that we never hear of the huge American study which showed that women who eat lots of veggies have an INCREASED risk of stomach cancer? So the official recommendation to eat five lots of veggies every day might just be creating lots of cancer for the future! It's as plausible (i.e. not very) as all the other dietary "wisdom" we read about fat etc.
10). And will "this generation of Western children be the first in history to lead shorter lives than their parents did"? This is another anti-fat scare that emanates from a much-cited editorial in a prominent medical journal that said so. Yet this editorial offered no statistical basis for its opinion -- an opinion that flies directly in the face of the available evidence.
Even statistical correlations far stronger than anything found in medical research may disappear if more data is used. A remarkable example from Sociology:"The modern literature on hate crimes began with a remarkable 1933 book by Arthur Raper titled The Tragedy of Lynching. Raper assembled data on the number of lynchings each year in the South and on the price of an acre's yield of cotton. He calculated the correlation coefficient between the two series at -0.532. In other words, when the economy was doing well, the number of lynchings was lower.... In 2001, Donald Green, Laurence McFalls, and Jennifer Smith published a paper that demolished the alleged connection between economic conditions and lynchings in Raper's data. Raper had the misfortune of stopping his analysis in 1929. After the Great Depression hit, the price of cotton plummeted and economic conditions deteriorated, yet lynchings continued to fall. The correlation disappeared altogether when more years of data were added."So we must be sure to base our conclusions on ALL the data. But in medical research, data selectivity and the "overlooking" of discordant research findings is epidemic.
"What we should be doing is monitoring children from birth so we can detect any deviations from the norm at an early stage and action can be taken". Who said that? Joe Stalin? Adolf Hitler? Orwell's "Big Brother"? The Spanish Inquisition? Generalissimo Francisco Franco Bahamonde? None of those. It was Dr Colin Waine, chairman of Britain's National Obesity Forum. What a fine fellow!
*********************
25 March, 2008
Damage to unborn baby from smoking 'negligible' in the first five months
This is a nice bit of iconoclasm. Rather in line with the passive smoking findings, too. The authors even managed to reject the "correlation is causation" belief that seems to pervade medical research. Will wonders never cease?
Smoking in pregnancy is far less damaging to the unborn baby than commonly supposed, detailed analysis suggests. If women give up smoking by the fifth month of pregnancy, the effect on the baby is negligible, the study found. And even if they do not, the effect on birthweight is surprisingly small. The study by Emma Tominey, a research assistant at the Centre for Economic Performance at the London School of Economics, throws new light on government efforts to stop women smoking when they become pregnant. While it does not suggest that such efforts are pointless, it shows that directing advice towards the newly pregnant is worthwhile.
It also shows that the worst effects are suffered by women from the poorest backgrounds, because in their case smoking is often combined with other unhealthy activities, such as poor diet and consumption of alcohol. Middle-class women suffer almost no damaging effects, the analysis suggests, even if they continue to smoke throughout pregnancy.
The findings, published as a report by the centre, will not be welcomed by anti-smoking groups, whose message to young women is intended to make them feel guilty about damaging their babies. In Ms Tominey's view, the damage is real but relatively small, and even if all women gave up smoking, only about one in eight babies with a low birthweight would avoid being classified as such.
The report uses data from the UK National Child Development Study, which provides details of mothers and their children between 1973 and 2000 - a total of 3,368 women and 6,860 children. The information includes the mothers' smoking habits, information about their families, and the birthweight and gestation period of the children.
Analysis of the data shows that smoking throughout pregnancy reduces birthweight by 5.6 per cent, and the gestation period by just over a day. But when the results are corrected for other factors, such as diet, lifestyle and alcohol, the effect of smoking on birthweight drops to 1.8 per cent and the reduction in gestation becomes insignificant. The study also finds that, contrary to the normal belief that damage is done early in pregnancy, it is the final third that matters most, because this is when babies gain the most weight.
Another surprising finding is the strong class effect. The damage is greatest among mothers with the lowest levels of education. Those who leave school at 16 cause twice the harm to their babies with each cigarette smoked. Ms Tominey concludes: "Other behaviours of the mother play a large role . . . over and above her smoking habits." Policies intended to help babies should aim to educate mothers generally, not simply try to persuade them to stop smoking, she said.
However, she does not conclude that smoking is harmless. "We find that up to 13 per cent of children classified as low-birthweight born to smoking mothers could have been classified as healthy, had their mothers not smoked." The policy implications, however, are that stopping smoking alone is not enough to deal with inequalities in child health, she concludes. "Not only is it the low-socioeconomic-status mothers who choose to smoke, but they are also the mothers bearing the greatest burden from the smoking." She said: "Therefore, any potential solution must offer help to these mothers, to target those with the worst habits and poorest records of child health."
Source
Wow! Big risk from "old" blood
This rather amplifies my comments about transfusions in the side-column. People are finally doing research into transfusions -- and entrenched assumptions are falling like ninepins
Thousands of heart surgery patients may be at risk from transfusions of blood that has been stored for two weeks or more. A study of more than 9,000 patients in the US has shown that those given blood more than 14 days old are 65 per cent more likely to die before discharge, and 50 per cent more likely to die within a year. Recipients of older blood are also at much higher risk of blood poisoning and multi-organ failure, according to the survey at the Cleveland Clinic in Ohio.
Blood is usually more than ten days old before it even reaches British hospitals, so patients here are at least as likely as those in America to receive blood that is more than two weeks old. As there are at least 30,000 cardiac operations a year in Britain, half involving blood transfusions, many patients could be at risk. Professor Peter Weissberg, the medical director of the British Heart Foundation, said that the safety of blood transfusions given to heart surgery patients should urgently be reviewed. "This research suggests that the longer transfused blood has been stored, the greater the risk of complications following cardiac surgery. Further research is urgently needed to clarify the indications for transfusion and the effects of blood storage on outcome," he said.
He said that research carried out for his foundation in Bristol last year indicated that many transfusions given to heart patients did more harm than good. "Together, these studies suggest that only those whose lives are at serious risk without a transfusion should receive blood," he said.
The Cleveland Clinic researchers, writing in The New England Journal of Medicine, say that changes are needed urgently to prevent unnecessary deaths among this large but vulnerable group of patients. According to Colleen Koch, the lead researcher, the results suggest "that blood should be classified as outdated earlier than current recommendations". On the basis of earlier laboratory studies, Dr Koch speculates that by the age of two weeks the structure of stored red blood cells has begun to break down. This, she says, may increase the risk that they will block blood vessels and reduce their capacity to carry oxygen.
Her team studied the records of patients who had major heart surgery at the hospital between June 1998 and January 2006. A total of 2,872 patients received blood that had been stored for 14 days or less, and 3,130 patients received blood that was more than 14 days old. The mean storage age was 11 days for the newer blood and 20 days for the older blood.
The number dying in hospital was significantly higher among those who were given older blood: 2.8 per cent compared with 1.7 per cent, while death rates a year on, at 11 per cent, were nearly half as high again as those who were given newer blood (7.4 per cent). There was no significant difference in the amount of blood received by the patients in the two groups.
Gavin Murphy, a senior lecturer in cardiac surgery at the University of Bristol who led last year's British Heart Foundation study, said that the routine use of transfusions for heart surgery patients put them in danger and was a huge drain on resources. Giving transfusions and treating transfusion-related illnesses increased the overall cost of staying in hospital by more than 40 per cent.
Source
****************
Just some problems with the "Obesity" war:
1). It tries to impose behavior change on everybody -- when most of those targeted are not obese and hence have no reason to change their behaviour. It is a form of punishing the innocent and the guilty alike. (It is also typical of Leftist thinking: Scorning the individual and capable of dealing with large groups only).
2). The longevity research all leads to the conclusion that it is people of MIDDLING weight who live longest -- not slim people. So the "epidemic" of obesity is in fact largely an "epidemic" of living longer.
3). It is total calorie intake that makes you fat -- not where you get your calories. Policies that attack only the source of the calories (e.g. "junk food") without addressing total calorie intake are hence pissing into the wind. People involuntarily deprived of their preferred calorie intake from one source are highly likely to seek and find their calories elsewhere.
4). So-called junk food is perfectly nutritious. A big Mac meal comprises meat, bread, salad and potatoes -- which is a mainstream Western diet. If that is bad then we are all in big trouble.
5). Food warriors demonize salt and fat. But we need a daily salt intake to counter salt-loss through perspiration and the research shows that people on salt-restricted diets die SOONER. And Eskimos eat huge amounts of fat with no apparent ill-effects. And the average home-cooked roast dinner has LOTS of fat. Will we ban roast dinners?
6). The foods restricted are often no more calorific than those permitted -- such as milk and fruit-juice drinks.
7). Tendency to weight is mostly genetic and is therefore not readily susceptible to voluntary behaviour change.
8). And when are we going to ban cheese? Cheese is a concentrated calorie bomb and has lots of that wicked animal fat in it too. Wouldn't we all be better off without it? And what about butter and margarine? They are just about pure fat. Surely they should be treated as contraband in kids' lunchboxes! [/sarcasm].
9). And how odd it is that we never hear of the huge American study which showed that women who eat lots of veggies have an INCREASED risk of stomach cancer? So the official recommendation to eat five lots of veggies every day might just be creating lots of cancer for the future! It's as plausible (i.e. not very) as all the other dietary "wisdom" we read about fat etc.
10). And will "this generation of Western children be the first in history to lead shorter lives than their parents did"? This is another anti-fat scare that emanates from a much-cited editorial in a prominent medical journal that said so. Yet this editorial offered no statistical basis for its opinion -- an opinion that flies directly in the face of the available evidence.
Even statistical correlations far stronger than anything found in medical research may disappear if more data is used. A remarkable example from Sociology:"The modern literature on hate crimes began with a remarkable 1933 book by Arthur Raper titled The Tragedy of Lynching. Raper assembled data on the number of lynchings each year in the South and on the price of an acre's yield of cotton. He calculated the correlation coefficient between the two series at -0.532. In other words, when the economy was doing well, the number of lynchings was lower.... In 2001, Donald Green, Laurence McFalls, and Jennifer Smith published a paper that demolished the alleged connection between economic conditions and lynchings in Raper's data. Raper had the misfortune of stopping his analysis in 1929. After the Great Depression hit, the price of cotton plummeted and economic conditions deteriorated, yet lynchings continued to fall. The correlation disappeared altogether when more years of data were added."So we must be sure to base our conclusions on ALL the data. But in medical research, data selectivity and the "overlooking" of discordant research findings is epidemic.
"What we should be doing is monitoring children from birth so we can detect any deviations from the norm at an early stage and action can be taken". Who said that? Joe Stalin? Adolf Hitler? Orwell's "Big Brother"? The Spanish Inquisition? Generalissimo Francisco Franco Bahamonde? None of those. It was Dr Colin Waine, chairman of Britain's National Obesity Forum. What a fine fellow!
*********************
24 March, 2008
Drinking while pregnant risks autism in babies
This report is OK as far as it goes. There is no doubt that heavy drinking during pregnancy is harmful to the fetal brain and that the damage could in part manifest as autistic symptoms is no surprise. Note however that autism sufferers are often high-functioning in some ways and that is not characteristic of fetal alcohol sufferers. These findings are not then relevant to autism research in general. All they do is add symptoms to fetal alcohol syndrome
Women who drink alcohol during pregnancy may be putting their babies at risk of developing autism, according to new research. The consultant psychiatrist who alerted the medical profession to the finding that drinking while pregnant can give babies a condition called foetal alcohol syndrome (FAS) has now found that the consumption of alcohol by expecting mothers can also cause autism. The research is the first to suggest that autism may be triggered by the child's mother drinking alcohol during pregnancy. The findings will heighten concern about the increase in alcohol consumption among women of childbearing age.
More than half of all mothers drink alcohol while pregnant, according to the Department of Health. This week the National Institute for Health and Clinical Excellence will issue a new warning about the dangers. A recent survey showed 8% of women aged 18 to 24 had consumed at least 35 units of alcohol, the equivalent of about 15 glasses of wine, during the previous week. Binge drinking among young women has resulted in the number of alcohol-related deaths in women aged 35 to 54 doubling between 1991 and 2005. Earlier this year, the British Medical Association warned that the increase in alcohol consumption by young women will be reflected in a rise in drinking during pregnancy and, subsequently, will put more babies at risk of being damaged by alcohol while in the womb.
Raja Mukherjee, consultant psychiatrist at Surrey Borders Partnership NHS trust, has spent the past 18 months examining children who have been damaged by their mother's drinking during pregnancy and found that a high proportion of them have autism. The research has been presented at scientific meetings. Mukherjee, who has presented his findings to medical colleagues, declined to discuss them in detail before their publication in a medical journal but said: "Genetic conditions are by far the most common cause of autism but that is not to say that other things cannot cause it, and prenatal alcohol appears, possibly, to be [a cause]. "Unlike genetic conditions, this is 100% preventable."
Mukherjee has previously warned against any drinking during pregnancy and believes that even low levels of alcohol may endanger babies. Drinking during pregnancy can cause foetal alcohol spectrum disorder, the umbrella term for a range of disorders - from minor anomalies such as low birth weight to severe FAS, the symptoms of which include mental retardation and facial abnormalities such as a short nose. The number of cases of FAS in Britain has increased in recent years. So far the government and medical bodies have given out conflicting messages about how much alcohol it is safe to drink during pregnancy.
Source
Hope for type 1 diabetes cure
RESEARCHERS are a step closer to a cure for type 1 diabetes after the successful transplantation of insulin-producing cells into eight patients. The breakthrough gives hope to the 140,000 Australians, who survive on daily insulin injections. Wayne Hawthorne, from the national pancreas and islet transplant unit at Westmead Hospital, said the experimental procedure might soon be a real option for everyone with type 1 diabetes, including children.
Scientists transplanted the insulin-producing islet cells from a donor pancreas into the patients' livers, where they began to produce insulin. In people who have type 1 diabetes, the body's immune system malfunctions, producing an auto-immune response that destroys these cells. After one treatment, the amount of insulin the patients needed to control blood glucose levels was dramatically reduced, in some cases to zero.
Mike Wilson, the chief executive of the Juvenile Diabetes Research Foundation in Australia, said the treatment effectively reversed diabetes. "This is an incredibly exciting step forward for both the type 1 diabetes community and for the world-class Australian researchers who are rapidly advancing in this area," he said.
Only patients with brittle (unstable) diabetes, where blood sugar drops dramatically without warning, have been treated so far, but Dr Hawthorne said the aim was to treat everyone with the disease. However, he said low organ donation rates meant islet transplants would remain out of reach unless another way to source the cells was found.
Fewer than 90 pancreases become available a year for this type of operation in Australia but more than 2000 people are newly diagnosed with type 1 diabetes. Xenotransplantation, where animal cells are transplanted into humans, is an option being investigated. Last month scientists in the United States turned stem cells into insulin producers that responded to blood glucose levels. Islet cell transplants have been reliable and viable only in the past few years because there have been major scientific advances. About 200 patients worldwide have been treated, with 80 per cent of them not needing insulin injections 12 months later.
However, patients need potentially toxic immuno-suppressant drugs so their bodies do not reject the new cells, and the drugs have serious side effects that for some people are worse than the disease.
Last week collaborating researchers at St Vincent's Institute of Medical Research in Melbourne announced the successful transplantation of insulin-producing islet cells into a Victorian woman. Elaine Robinson, 54, no longer sufferers from life-threatening hypoglycaemic attacks and needs to inject only a small fraction of the amount of insulin she was using previously. A planned second transplant could eliminate the need for insulin completely.
Source
****************
Just some problems with the "Obesity" war:
1). It tries to impose behavior change on everybody -- when most of those targeted are not obese and hence have no reason to change their behaviour. It is a form of punishing the innocent and the guilty alike. (It is also typical of Leftist thinking: Scorning the individual and capable of dealing with large groups only).
2). The longevity research all leads to the conclusion that it is people of MIDDLING weight who live longest -- not slim people. So the "epidemic" of obesity is in fact largely an "epidemic" of living longer.
3). It is total calorie intake that makes you fat -- not where you get your calories. Policies that attack only the source of the calories (e.g. "junk food") without addressing total calorie intake are hence pissing into the wind. People involuntarily deprived of their preferred calorie intake from one source are highly likely to seek and find their calories elsewhere.
4). So-called junk food is perfectly nutritious. A big Mac meal comprises meat, bread, salad and potatoes -- which is a mainstream Western diet. If that is bad then we are all in big trouble.
5). Food warriors demonize salt and fat. But we need a daily salt intake to counter salt-loss through perspiration and the research shows that people on salt-restricted diets die SOONER. And Eskimos eat huge amounts of fat with no apparent ill-effects. And the average home-cooked roast dinner has LOTS of fat. Will we ban roast dinners?
6). The foods restricted are often no more calorific than those permitted -- such as milk and fruit-juice drinks.
7). Tendency to weight is mostly genetic and is therefore not readily susceptible to voluntary behaviour change.
8). And when are we going to ban cheese? Cheese is a concentrated calorie bomb and has lots of that wicked animal fat in it too. Wouldn't we all be better off without it? And what about butter and margarine? They are just about pure fat. Surely they should be treated as contraband in kids' lunchboxes! [/sarcasm].
9). And how odd it is that we never hear of the huge American study which showed that women who eat lots of veggies have an INCREASED risk of stomach cancer? So the official recommendation to eat five lots of veggies every day might just be creating lots of cancer for the future! It's as plausible (i.e. not very) as all the other dietary "wisdom" we read about fat etc.
10). And will "this generation of Western children be the first in history to lead shorter lives than their parents did"? This is another anti-fat scare that emanates from a much-cited editorial in a prominent medical journal that said so. Yet this editorial offered no statistical basis for its opinion -- an opinion that flies directly in the face of the available evidence.
Even statistical correlations far stronger than anything found in medical research may disappear if more data is used. A remarkable example from Sociology:"The modern literature on hate crimes began with a remarkable 1933 book by Arthur Raper titled The Tragedy of Lynching. Raper assembled data on the number of lynchings each year in the South and on the price of an acre's yield of cotton. He calculated the correlation coefficient between the two series at -0.532. In other words, when the economy was doing well, the number of lynchings was lower.... In 2001, Donald Green, Laurence McFalls, and Jennifer Smith published a paper that demolished the alleged connection between economic conditions and lynchings in Raper's data. Raper had the misfortune of stopping his analysis in 1929. After the Great Depression hit, the price of cotton plummeted and economic conditions deteriorated, yet lynchings continued to fall. The correlation disappeared altogether when more years of data were added."So we must be sure to base our conclusions on ALL the data. But in medical research, data selectivity and the "overlooking" of discordant research findings is epidemic.
"What we should be doing is monitoring children from birth so we can detect any deviations from the norm at an early stage and action can be taken". Who said that? Joe Stalin? Adolf Hitler? Orwell's "Big Brother"? The Spanish Inquisition? Generalissimo Francisco Franco Bahamonde? None of those. It was Dr Colin Waine, chairman of Britain's National Obesity Forum. What a fine fellow!
*********************
23 March, 2008
Fertility Treatment is Hugely Successful but Largely Ignored by Medicine
I know nothing about the procedures promoted below but pass this on in case there are readers who want to look in to it. I tend to have a kneejerk reaction in favor of anything that has apparently been censored
NaProTECHNOLOGY (Natural Procreative Technology or NPT) is a dramatically successful, but not well known or practiced method of diagnosing and treating gynecological diseases and infertility in women. It is a morally acceptable and very cost effective method of restoring fertility, using a fertility-care based medical approach, rather than a fertility-control approach.
This new reproductive science works cooperatively with the natural fertility [menstrual] cycle. It has been developed as a series of medical applications based on a standardized assessment of the biomarkers of the fertility [menstrual] cycle, known as the Creighton Model FertilityCare System. It can be used to evaluate and treat infertility, miscarriage, irregular cycles, ovarian cysts, premenstrual syndrome, postpartum depression and many other women's health conditions.
When used to treat infertility alone, NaProTechnology has a success rate of 76% in assisting couples to achieve pregnancy - remarkably superior to the 10-15% success rate of in vitro fertilization, and without the enormous financial cost and adverse emotional and other psychological effects of in vitro fertilization.
NPT was developed from thirty years of scientific research in the study of the normal and abnormal states of the menstrual and fertility cycles by Dr. Thomas W. Hilgers, director of the Pope Paul VI Institute for the Study of Human Reproduction and the National Center for Women's Health in Omaha, Nebraska. Dr. Hilgers is currently a senior medical consultant in obstetrics, gynecology, and reproductive medicine and surgery at the Pope Paul VI Institute and a clinical professor in the Department of Obstetrics and Gynecology at Creighton University School of Medicine.
According to Dr. John B. Shea, medical consultant for LifeSiteNews.com, NPT has not been accepted by the majority of the medical profession because "in reference to female infertility, NPT competes against a well financed option, in vitro fertilization [IVF], that is already deeply entrenched in the marketplace and in political circles."
"Furthermore, physicians who might be interested in NPT experience a lot of peer pressure to view NPT as an oddball kind of medical care simply because they had not heard of it in medical school," Dr. Shea explained. "Also, since NPT originated in the Pope Paul VI Institute, there may also be an element of anti-Catholic bias and an element of 'go-along-to-get-along' pressure involved."
The American Society for Reproductive Medicine (ASRM), which maintains a fully staffed Office of Public Affairs in Washington D.C., and a web site that contains a vast amount of information on reproductive matters, does not have any information on NPT posted on its website. Chuck Weber has reported that a spokesperson for ASRM, when asked to comment on NPT, declined to comment, saying, "We tend to just ignore these people".
Source
Censorship built on junk arguments
The global campaign to ban junk food ads is based on junk science: there's little evidence children 'eat what they watch'. Patrick Basham and John Luik, co-authors of Diet Nation: Exposing the Obesity Crusade, say it is folly to try to change people's diets and waistlines by banning ads for fatty foods.
A new global campaign to restrict junk food advertising to children is the public health equivalent of using a cricket bat to swat a fly. Such a ban would not just be an over-the-top, crude policy instrument - it is also deeply unscientific.
In the UK, there is currently a ban on such junk food adverts during television programmes that have a `particular appeal' to under-16s. The ban covers both programmes and channels aimed specifically at kids, and other programmes that have a relatively high audience of children. The aim of the new campaign, spearheaded by the London-based International Obesity Task Force (IOTF), is to go further than this: to ban television advertising between 6am and 9pm for foods high in fat, sugar and salt; to completely ban internet and new media advertising; and to prohibit the use of celebrities or cartoon characters, competitions and free gifts to promote `junk food'.
The IOTF's rationale rests upon a series of influential recent reports by the American Psychological Association, the US Institute of Medicine, the UK Food Standards Agency, and the UK television regulator, Ofcom. These reports claim that food advertising to children causes them to eat a diet that makes them overweight or obese. Consequently, it is alleged that restrictions on food advertising will reduce weight problems and obesity amongst young people.
If you peek behind the regulatory curtain, however, the claims about the causal influences of food advertising on children's diets and weight share a central and definitive flaw in their understanding of what counts as demonstrating causality. In order to establish an evidence-based case for food advertising as a cause of childhood overweight and obesity, one would have to demonstrate that such advertising had an independent effect on children's weight. This, in turn, would require a research study design that controlled for the multiple other risk factors (by some estimates dozens) connected with childhood obesity.
However, none of the studies purporting to demonstrate that food advertising causes childhood obesity control for more than a handful of these other risk factors. These studies therefore cannot establish an evidence-based case about the connection between food advertising and children's weight.
If food advertising caused children's weight gain and obesity, wouldn't you expect to find an increase in advertising that parallels the increase in obesity? This is not the case. UK food and drink ad spending has been falling in real terms since 1999 and is now roughly at 1982 levels, even while rates of overweight and obesity have been rising. Consider, too, that in 1982 food ads constituted 34 per cent of total television advertising, whereas in 2002 they made up only 18 per cent.
In the US, one finds a similar trend. According to the Federal Trade Commission, advertising during children's TV programming has declined by 34 per cent in recent years. Data from Nielsen surveys shows that food advertising on television has declined by 13 per cent since 1993.
If the level of advertising has not increased, perhaps the level of TV viewing has gone up? In fact, to the surprise of many, TV viewing has not increased during the period of the obesity `epidemic', and some observers suggest that it has not changed for children and adolescents for the past 40 years. There is some evidence that the time children spend watching TV has actually declined in recent years.
Furthermore, when children sit down to watch TV, they actually view a balanced presentation of foods. A unique British study looked at the food references and messages in regular programming, as opposed to those contained in food advertising. There were as many references to food within regular programming as during the adverts. Children's regular food programming contained references far more centred on so-called healthy foods. For example, fruit and vegetables were the most frequently portrayed foods in regular programming.
The IOTF will not tell you this, but there is also no proven connection between food advertising and food consumption patterns. There is a substantial econometric literature that disproves the alleged connection between advertising, diets and weight. Peter Kyle of the University of Lancaster examined the impact of food advertising on food consumption and found no evidence to support the popular myth that advertising will increase market size.
Martyn Duffy of the University of Manchester studied the impact of advertising on 11 food categories. Not only did advertising have no effect on food demand, but it also had virtually no effect on the demand for any individual food. Duffy's conclusions are hardly exceptional. Other studies into the effect of advertising of such items as breakfast cereals and biscuits, both frequently cited as bogeymen in the childhood obesity epidemic, have concluded that advertising did not affect market size in any general way or to any material extent.
Bob Eagle and Tim Ambler looked at the impact of advertising on chocolate consumption in five European countries in order to test the claim that a reduction in advertising would reduce consumption. They report no significant association between the amount of advertising and the size of the chocolate market. Eagle and Ambler's work is corroborated by evidence from the Canadian province of Quebec and from Sweden, both of which have had advertising bans on foods to children, Quebec since 1980. In both jurisdictions, however, there have not been significant reductions in childhood obesity or marked differences in obesity rates compared with other adjacent areas.
Brian Young of Exeter University studied the effects of food advertising on children's food choices for the Ministry of Agriculture, Fisheries and Food. Young found that children's food acceptance patterns and eating preferences develop in infancy. Therefore, they predate the influence of advertising. If children do prefer foods that are sweet, high in fat and salty, it is not because advertising created those preferences.
Despite the highly publicised claims to the contrary, the scientific evidence fails to provide a causal link between food advertising and children's eating patterns or weight. You cannot expect parents pushing their supermarket trolleys to be aware of this inconvenient truth. But the IOTF has no excuse for hauling obesity policy into this evidence-free zone.
Source
****************
Just some problems with the "Obesity" war:
1). It tries to impose behavior change on everybody -- when most of those targeted are not obese and hence have no reason to change their behaviour. It is a form of punishing the innocent and the guilty alike. (It is also typical of Leftist thinking: Scorning the individual and capable of dealing with large groups only).
2). The longevity research all leads to the conclusion that it is people of MIDDLING weight who live longest -- not slim people. So the "epidemic" of obesity is in fact largely an "epidemic" of living longer.
3). It is total calorie intake that makes you fat -- not where you get your calories. Policies that attack only the source of the calories (e.g. "junk food") without addressing total calorie intake are hence pissing into the wind. People involuntarily deprived of their preferred calorie intake from one source are highly likely to seek and find their calories elsewhere.
4). So-called junk food is perfectly nutritious. A big Mac meal comprises meat, bread, salad and potatoes -- which is a mainstream Western diet. If that is bad then we are all in big trouble.
5). Food warriors demonize salt and fat. But we need a daily salt intake to counter salt-loss through perspiration and the research shows that people on salt-restricted diets die SOONER. And Eskimos eat huge amounts of fat with no apparent ill-effects. And the average home-cooked roast dinner has LOTS of fat. Will we ban roast dinners?
6). The foods restricted are often no more calorific than those permitted -- such as milk and fruit-juice drinks.
7). Tendency to weight is mostly genetic and is therefore not readily susceptible to voluntary behaviour change.
8). And when are we going to ban cheese? Cheese is a concentrated calorie bomb and has lots of that wicked animal fat in it too. Wouldn't we all be better off without it? And what about butter and margarine? They are just about pure fat. Surely they should be treated as contraband in kids' lunchboxes! [/sarcasm].
9). And how odd it is that we never hear of the huge American study which showed that women who eat lots of veggies have an INCREASED risk of stomach cancer? So the official recommendation to eat five lots of veggies every day might just be creating lots of cancer for the future! It's as plausible (i.e. not very) as all the other dietary "wisdom" we read about fat etc.
10). And will "this generation of Western children be the first in history to lead shorter lives than their parents did"? This is another anti-fat scare that emanates from a much-cited editorial in a prominent medical journal that said so. Yet this editorial offered no statistical basis for its opinion -- an opinion that flies directly in the face of the available evidence.
Even statistical correlations far stronger than anything found in medical research may disappear if more data is used. A remarkable example from Sociology:"The modern literature on hate crimes began with a remarkable 1933 book by Arthur Raper titled The Tragedy of Lynching. Raper assembled data on the number of lynchings each year in the South and on the price of an acre's yield of cotton. He calculated the correlation coefficient between the two series at -0.532. In other words, when the economy was doing well, the number of lynchings was lower.... In 2001, Donald Green, Laurence McFalls, and Jennifer Smith published a paper that demolished the alleged connection between economic conditions and lynchings in Raper's data. Raper had the misfortune of stopping his analysis in 1929. After the Great Depression hit, the price of cotton plummeted and economic conditions deteriorated, yet lynchings continued to fall. The correlation disappeared altogether when more years of data were added."So we must be sure to base our conclusions on ALL the data. But in medical research, data selectivity and the "overlooking" of discordant research findings is epidemic.
"What we should be doing is monitoring children from birth so we can detect any deviations from the norm at an early stage and action can be taken". Who said that? Joe Stalin? Adolf Hitler? Orwell's "Big Brother"? The Spanish Inquisition? Generalissimo Francisco Franco Bahamonde? None of those. It was Dr Colin Waine, chairman of Britain's National Obesity Forum. What a fine fellow!
*********************
22 March, 2008
THAT MAGICAL VITAMIN D AGAIN
The popular report immediately below is much less cautious than the original journal article, also reproduced. It would appear that the effects are small and the type of data weak
Note that Vitamin D has also recently been shown to be bad for you. Note also here, where antioxidants generally were found to be bad for you.
Children given vitamin D supplements have a lower risk of developing type 1 diabetes, says a study in the Archives of Disease in Childhood. Type 1 diabetes is when the body's immune system attacks and destroys cells in the pancreas that produce insulin. Without insulin, cells are unable to take up sugar from the blood that they need to function properly. The authors combined information from five studies looking at the effect of vitamin D supplements on the risk of type 1 diabetes. Overall, children given extra vitamin D in the form of tablets or cod liver oil were 29 per cent less likely to develop type 1 diabetes compared to children who were not given supplements. The higher and more regular the dose, the lower the chances of developing the disease. Clinical trials are now needed, say the authors, to find out which form and dose of vitamin D gives the best protection, and at what age it should be given to children.
Source
Vitamin D Supplementation in Early Childhood and Risk of Type 1 Diabetes: a Systematic Review and Meta-analysis
By Christos S. Zipitis et al.
Objectives: To assess whether vitamin D supplementation in infancy reduces risk of type 1 diabetes in later life.
Design: Systematic review and meta-analysis. Data sources: Medline, Embase, Cinahl, Cochrane Central Register of Controlled Trials and reference lists of retrieved articles.
Main outcome measure: Development of type 1 diabetes.
Inclusion criteria: Controlled trials and observational studies which had assessed the effect of vitamin D supplementation on risk of developing type 1 diabetes.
Results: Five observational studies met the inclusion criteria; no randomised controlled trials were found. 4 of the 5 included studies were case control studies and the fifth study was a cohort study. Meta-analysis of data from the case control studies showed that the risk of type 1 diabetes was significantly reduced in infants who were supplemented with vitamin D compared to those who were not supplemented (pooled odds ratio 0.71, 95% CI 0.60 to 0.84). The result of the cohort study was in agreement with that of the meta-analysis. There was also some evidence of a dose-response effect, with those using higher amounts of vitamin D being at lower risk of developing type 1 diabetes. Finally, there was a suggestion that the timing of supplementation might also be important for the subsequent development of type 1 diabetes.
Conclusion: Vitamin D supplementation in early childhood may offer protection against the development of type 1 diabetes. The evidence for this is based on observational studies. Adequately powered, randomised controlled trials with long periods of follow-up are needed to establish causality and the best formulation, dose, duration and period of supplementation.
Arch Dis Child. 13 March 2008
Passive smoking
I personally detest having the air I breathe polluted by tobacco smoke. It once used to happen a lot but is now rare because of the various prohibitions on smoking that have gradually been legislated throughout the Western world. I am extremely grateful about that.
The prohibitions were gradually put in place on the back of a claim that exposure to smoke from others is bad for your health. I think there is now a widespread recognition that such a claim is rubbish. I believe that the bans were justifiable as just another curb on offensive behaviour but they are not justifiable on medical grounds. We now see a similar dishonest attack on obesity. Obesity is aethetically offensive but to curb it you have to pretend that it is medically harmful. It is not.
So just for the record I reproduce below a background article on the passive smoking plus the abstract of what is probably the most solid of the research on passive smoking. It involved a very large number of people over a very long period of time and found no significant effect of passive smoking. I understand that the authors encountered difficulty in getting the paper published, due to its unpopular conclusions.All done with passive smoke and mirrorsAnd the most significant scientific report:
Anti-smoking activists can celebrate today one of the most remarkable lobbying campaigns in modern politics. The statutory no-smoking signs outside every "enclosed public space", including churches, synagogues, mosques and Buckingham Palace, will always remind us how they find the smell of other people's smoke offensive. One thing they cannot claim, though, is that protecting people from others' smoke will save thousands of lives.
The scientific evidence to support their belief that inhaling other people's smoke causes cancer simply does not exist. In the course of writing a book on "scares", I recently trawled through all the scientific literature on the health risks of tobacco, ever since Richard Doll's seminal paper in 1950 alerted the world to the link between smoking and lung cancer (when 82 per cent of British men were smokers). Over the next 30 years, the realisation that smokers risked serious damage to their health led to a 50 per cent drop in the habit. But this divided people into three groups: more or less addicted smokers, generally tolerant non-smokers and fiercely intolerant anti-smokers.
At the end of the Seventies, the anti-smokers first seriously turned their attention to what they called "passive smoking". Over the next decade, it is fascinating to follow how, try as they might, they could not come up with the evidence they wanted to prove that "environmental tobacco smoke" was directly harming non-smokers' health. They became greatly excited by a series of studies which purported to show a link between smoking and cot deaths. But these somehow managed to ignore the fact that, in the very years when cot deaths were rising by 500 per cent, the incidence of smoking had halved.
A further series of studies in the Nineties, mainly in the US, claimed to have found that passive smoking was causing thousands of deaths a year. But however much the researchers tried to manipulate the evidence, none could come up with an increased risk of cancer that, by the strict rules of epidemiology, was "statistically significant".
In 1998 and 2003 came the results of by far the biggest studies of passive smoking ever carried out. One was conducted by the International Agency for Research on Cancer, part of the World Health Organisation. The other, run by Prof James Enstrom and Geoffrey Kabat for the American Cancer Society, was a mammoth 40-year-long study of 35,000 non-smokers living with smokers. In each case, when the sponsors saw the results they were horrified. The evidence inescapably showed that passive smoking posed no significant risk. This confirmed Sir Richard Doll's own comment in 2001: "The effects of other people's smoking in my presence is so small it doesn't worry me".
In each case, the sponsors tried to suppress the results, which were only with difficulty made public (the fact that Enstrom and Kabat, both non-smokers, could only get their results published with help from the tobacco industry was inevitably used to discredit them, even though all their research had been financed by the anti-tobacco cancer charity).
In the early years of this decade, the anti-smokers had become so carried away by the rightness of their cause that they no longer worried about finding disciplined evidence for their statistical claims. One notorious but widely-quoted study commissioned by 33 councils campaigning for a "smoke-free London" came up with the wonderfully precise claim that 617 Britons die each year from passive smoking in the workplace. No longer was there any pretence at serious debate. This was a propaganda war, in which statistics could be manufactured at will. (The European Commission's 2006 figure for annual deaths from passive smoking in the UK was around 12,000, some 20 times higher than the figure quoted by the British Government itself.)
By the time the Commons pushed through the smoking ban in February 2006, a kind of collective hysteria had taken over. MPs fell over themselves in boasting how many lives they were about to save. One Department of Health official was quoted as equating its significance to the Act setting up the National Health Service in 1948.
As clouds of self-righteousness billow out over England this weekend, the anti-smokers may be entitled to give us their view that smoking is a thoroughly noxious and nasty habit, even that it can exacerbate respiratory conditions such as asthma or bronchitis arising from other causes. They can even claim that the ban will save lives by persuading smokers to give up. But the one thing they cannot claim is any reliable evidence for their belief that passive smoking is responsible for killing people. Sir Richard Doll was right. It is merely a sanctimonious act of faith.
Source
Environmental tobacco smoke and tobacco related mortality in a prospective study of Californians, 1960-98.
By Enstrom JE & Kabat GC.
School of Public Health, University of California, Los Angeles, CA 90095-1772, USA. jenstrom@ucla.edu
OBJECTIVE: To measure the relation between environmental tobacco smoke, as estimated by smoking in spouses, and long term mortality from tobacco related disease.
DESIGN: Prospective cohort study covering 39 years.
SETTING: Adult population of California, United States.
PARTICIPANTS: 118 094 adults enrolled in late 1959 in the American Cancer Society cancer prevention study (CPS I), who were followed until 1998. Particular focus is on the 35 561 never smokers who had a spouse in the study with known smoking habits.
MAIN OUTCOME MEASURES: Relative risks and 95% confidence intervals for deaths from coronary heart disease, lung cancer, and chronic obstructive pulmonary disease related to smoking in spouses and active cigarette smoking.
RESULTS: For participants followed from 1960 until 1998 the age adjusted relative risk (95% confidence interval) for never smokers married to ever smokers compared with never smokers married to never smokers was 0.94 (0.85 to 1.05) for coronary heart disease, 0.75 (0.42 to 1.35) for lung cancer, and 1.27 (0.78 to 2.08) for chronic obstructive pulmonary disease among 9619 men, and 1.01 (0.94 to 1.08), 0.99 (0.72 to 1.37), and 1.13 (0.80 to 1.58), respectively, among 25 942 women. No significant associations were found for current or former exposure to environmental tobacco smoke before or after adjusting for seven confounders and before or after excluding participants with pre-existing disease. No significant associations were found during the shorter follow up periods of 1960-5, 1966-72, 1973-85, and 1973-98.
CONCLUSIONS: The results do not support a causal relation between environmental tobacco smoke and tobacco related mortality, although they do not rule out a small effect. The association between exposure to environmental tobacco smoke and coronary heart disease and lung cancer may be considerably weaker than generally believed.
Originally in The British Medical Journal, 2003;326:1057 (17 May). Also here
****************
Just some problems with the "Obesity" war:
1). It tries to impose behavior change on everybody -- when most of those targeted are not obese and hence have no reason to change their behaviour. It is a form of punishing the innocent and the guilty alike. (It is also typical of Leftist thinking: Scorning the individual and capable of dealing with large groups only).
2). The longevity research all leads to the conclusion that it is people of MIDDLING weight who live longest -- not slim people. So the "epidemic" of obesity is in fact largely an "epidemic" of living longer.
3). It is total calorie intake that makes you fat -- not where you get your calories. Policies that attack only the source of the calories (e.g. "junk food") without addressing total calorie intake are hence pissing into the wind. People involuntarily deprived of their preferred calorie intake from one source are highly likely to seek and find their calories elsewhere.
4). So-called junk food is perfectly nutritious. A big Mac meal comprises meat, bread, salad and potatoes -- which is a mainstream Western diet. If that is bad then we are all in big trouble.
5). Food warriors demonize salt and fat. But we need a daily salt intake to counter salt-loss through perspiration and the research shows that people on salt-restricted diets die SOONER. And Eskimos eat huge amounts of fat with no apparent ill-effects. And the average home-cooked roast dinner has LOTS of fat. Will we ban roast dinners?
6). The foods restricted are often no more calorific than those permitted -- such as milk and fruit-juice drinks.
7). Tendency to weight is mostly genetic and is therefore not readily susceptible to voluntary behaviour change.
8). And when are we going to ban cheese? Cheese is a concentrated calorie bomb and has lots of that wicked animal fat in it too. Wouldn't we all be better off without it? And what about butter and margarine? They are just about pure fat. Surely they should be treated as contraband in kids' lunchboxes! [/sarcasm].
9). And how odd it is that we never hear of the huge American study which showed that women who eat lots of veggies have an INCREASED risk of stomach cancer? So the official recommendation to eat five lots of veggies every day might just be creating lots of cancer for the future! It's as plausible (i.e. not very) as all the other dietary "wisdom" we read about fat etc.
10). And will "this generation of Western children be the first in history to lead shorter lives than their parents did"? This is another anti-fat scare that emanates from a much-cited editorial in a prominent medical journal that said so. Yet this editorial offered no statistical basis for its opinion -- an opinion that flies directly in the face of the available evidence.
Even statistical correlations far stronger than anything found in medical research may disappear if more data is used. A remarkable example from Sociology:"The modern literature on hate crimes began with a remarkable 1933 book by Arthur Raper titled The Tragedy of Lynching. Raper assembled data on the number of lynchings each year in the South and on the price of an acre's yield of cotton. He calculated the correlation coefficient between the two series at -0.532. In other words, when the economy was doing well, the number of lynchings was lower.... In 2001, Donald Green, Laurence McFalls, and Jennifer Smith published a paper that demolished the alleged connection between economic conditions and lynchings in Raper's data. Raper had the misfortune of stopping his analysis in 1929. After the Great Depression hit, the price of cotton plummeted and economic conditions deteriorated, yet lynchings continued to fall. The correlation disappeared altogether when more years of data were added."So we must be sure to base our conclusions on ALL the data. But in medical research, data selectivity and the "overlooking" of discordant research findings is epidemic.
"What we should be doing is monitoring children from birth so we can detect any deviations from the norm at an early stage and action can be taken". Who said that? Joe Stalin? Adolf Hitler? Orwell's "Big Brother"? The Spanish Inquisition? Generalissimo Francisco Franco Bahamonde? None of those. It was Dr Colin Waine, chairman of Britain's National Obesity Forum. What a fine fellow!
*********************
21 March, 2008
Smoking in pregnancy may affect child's personality (or not)
Boy, some medical researchers are in love with their assumptions. I would say that the data below shows that it is smoking MOTHERS who are more irritable. It is they who judge their children in the research below
Smoking in pregnancy not only passes harmful chemicals to the developing baby, but may also affect the child's personality.
In the Journal of Epidemiology and Community Health, researchers report that quitting smoking during pregnancy increases the chances of having an easy-going child. The findings are based on 18,819 UK babies.
Their mothers were classified according to smoking during pregnancy -- non-smokers, light smokers, heavy smokers (more than 10 cigarettes per day) or quitters. When their babies were nine months old, mothers were questioned in line with the widely-used Carey Infant Temperament Scale. The test scored on positive mood, receptivity to new things, and regular sleeping and eating patterns. Quitters had the most even-tempered babies, heavy smokers the most difficult.
J Epidemiol Community Health 2008;62:318-324 (Pickett KE, et al)
Source
Aspirin good for you (when it's not bad for you)
This study DOES seem to show that aspirin in beneficial for SOME asthma sufferers. As Aspirin is an anti-inflammatory, that is no great surprise. But should you take it? Aspirin DOES always cause some stomach bleeding! How does that sound?
Women on small doses of aspirin every second day are less likely to develop asthma, says a new study in Thorax. It suggests that low-dose aspirin could help to prevent asthma in some women who are at risk of developing the disease as adults. Researchers recruited 37,270 women aged 45 or over with no history of asthma. Half took 100 milligrams of aspirin every second day and the other half took a placebo. Every year for the next 10 years, participants were surveyed. There were 10 per cent fewer new cases of asthma in the aspirin group compared to the placebo group. While 963 placebo women developed asthma, only 872 women in the aspirin group developed the disease. Aspirin's protective effects were seen in women regardless of age, exercise or smoking, but not in obese women.
The authors caution that aspirin is known to worsen symptoms in around one in 10 people who have already been diagnosed with the disease.
Thorax, 2008. (Kurth T, et al)
Source
****************
Just some problems with the "Obesity" war:
1). It tries to impose behavior change on everybody -- when most of those targeted are not obese and hence have no reason to change their behaviour. It is a form of punishing the innocent and the guilty alike. (It is also typical of Leftist thinking: Scorning the individual and capable of dealing with large groups only).
2). The longevity research all leads to the conclusion that it is people of MIDDLING weight who live longest -- not slim people. So the "epidemic" of obesity is in fact largely an "epidemic" of living longer.
3). It is total calorie intake that makes you fat -- not where you get your calories. Policies that attack only the source of the calories (e.g. "junk food") without addressing total calorie intake are hence pissing into the wind. People involuntarily deprived of their preferred calorie intake from one source are highly likely to seek and find their calories elsewhere.
4). So-called junk food is perfectly nutritious. A big Mac meal comprises meat, bread, salad and potatoes -- which is a mainstream Western diet. If that is bad then we are all in big trouble.
5). Food warriors demonize salt and fat. But we need a daily salt intake to counter salt-loss through perspiration and the research shows that people on salt-restricted diets die SOONER. And Eskimos eat huge amounts of fat with no apparent ill-effects. And the average home-cooked roast dinner has LOTS of fat. Will we ban roast dinners?
6). The foods restricted are often no more calorific than those permitted -- such as milk and fruit-juice drinks.
7). Tendency to weight is mostly genetic and is therefore not readily susceptible to voluntary behaviour change.
8). And when are we going to ban cheese? Cheese is a concentrated calorie bomb and has lots of that wicked animal fat in it too. Wouldn't we all be better off without it? And what about butter and margarine? They are just about pure fat. Surely they should be treated as contraband in kids' lunchboxes! [/sarcasm].
9). And how odd it is that we never hear of the huge American study which showed that women who eat lots of veggies have an INCREASED risk of stomach cancer? So the official recommendation to eat five lots of veggies every day might just be creating lots of cancer for the future! It's as plausible (i.e. not very) as all the other dietary "wisdom" we read about fat etc.
10). And will "this generation of Western children be the first in history to lead shorter lives than their parents did"? This is another anti-fat scare that emanates from a much-cited editorial in a prominent medical journal that said so. Yet this editorial offered no statistical basis for its opinion -- an opinion that flies directly in the face of the available evidence.
Even statistical correlations far stronger than anything found in medical research may disappear if more data is used. A remarkable example from Sociology:"The modern literature on hate crimes began with a remarkable 1933 book by Arthur Raper titled The Tragedy of Lynching. Raper assembled data on the number of lynchings each year in the South and on the price of an acre's yield of cotton. He calculated the correlation coefficient between the two series at -0.532. In other words, when the economy was doing well, the number of lynchings was lower.... In 2001, Donald Green, Laurence McFalls, and Jennifer Smith published a paper that demolished the alleged connection between economic conditions and lynchings in Raper's data. Raper had the misfortune of stopping his analysis in 1929. After the Great Depression hit, the price of cotton plummeted and economic conditions deteriorated, yet lynchings continued to fall. The correlation disappeared altogether when more years of data were added."So we must be sure to base our conclusions on ALL the data. But in medical research, data selectivity and the "overlooking" of discordant research findings is epidemic.
"What we should be doing is monitoring children from birth so we can detect any deviations from the norm at an early stage and action can be taken". Who said that? Joe Stalin? Adolf Hitler? Orwell's "Big Brother"? The Spanish Inquisition? Generalissimo Francisco Franco Bahamonde? None of those. It was Dr Colin Waine, chairman of Britain's National Obesity Forum. What a fine fellow!
*********************
20 March, 2008
Doctors Use Estrogen to Treat Memory Loss in Older Women
Not that wicked "pill" again! The one that medical researchers do their best to discredit
Gayatri Devi was a neurologist and psychiatrist specializing in memory disorders when a patient's case changed her career. The 52-year Brazilian woman, once a dynamo, had become forgetful and disoriented. Dr. Devi and her colleagues diagnosed early Alzheimer's disease and prescribed a standard AD drug. As an afterthought, Dr. Devi added estrogen, having seen research suggesting it might slow the dreaded disease.
Six months later, the woman returned and insisted she was cured. "I didn't believe it, but we tested her and her symptoms had resolved, thanks to the estrogen," says Dr. Devi. "That was the beginning of my journey." In the 10 years since, Dr. Devi has treated several hundred patients for menopause-related memory loss in her New York City practice. Many are professional women who find they can't summon up words or lose track of what they were doing. Some are afraid to tell anyone, some have been dismissed as simply stressed. And some are still years away from menopause; the hormonal ups and down are often more pronounced in "perimenopause," which can start as much as seven years earlier. "They're terrified they are developing Alzheimer's disease," says Dr. Devi. "But the majority of them do respond to estrogen."
Other doctors who specialize in menopause say such cognitive problems are just as common as hot flashes and often more worrisome. "Women have been telling me this for 25 years," says Elizabeth Lee Vliet, a women's health physician with offices in Tucson, Ariz., and Dallas, Tex., who notes that her patients often speak of feeling "fuzzy-headed." She takes detailed blood tests and typically prescribes 17-beta estradiol, an FDA-approved estrogen replacement. "They come back a couple weeks later and say 'It was like someone turned a lightbulb on my brain! I can think again!' "
The phenomenon isn't surprising considering that there are estrogen receptors throughout the brain, particularly in the areas that govern learning, memory and mood. Estrogen also stimulates the growth of dendritic spines that enable nerve cells to communicate, and increases the level of neurotransmitters, the brain's chemical messengers In addition, estrogen helps regulate glucose, inflammation and antioxidants in the brain. Neuroimaging studies have shown that when estrogen declines, there is markedly less cerebral blood flow and activity.
Men's brains function differently. A 2005 study from the University of California at Irvine found that men rely much more heavily on gray matter, the information-processing centers in the brain, while women utilize more white matter, which provides networks between the processing centers. In short, women's brains make more connections. "Women remember word for word what somebody said yesterday, or last year," says Dr. Devi. But men's brains also require estrogen, which is converted from testosterone. In fact, because men continue to make testosterone all their lives, a 72-year old man typically has more estrogen than a 72-year old woman.
Many studies have confirmed that declining estrogen affects visual and verbal memory, language and other cognitive skills. Barbara Sherwin, a professor of psychology and ob/gyn at McGill University in Canada, has shown that women who had their ovaries removed surgically and were given estradiol -- the estrogen replacement that is the same as women lose -- scored significantly higher on tests of short- and long-term memory and verbal memory than women who had received placebos. In a study published in the Lancet in 1996, researchers at Columbia University found that elderly women who took estrogen replacement were 50% less likely to develop Alzheimer's disease later in life.
Other studies have found contradictory results -- most prominently, the Women's Health Initiative Memory Study (WHIMS), part of the big government hormone trial. It reported in 2004 that women taking estrogen plus progestin had a higher risk of dementia than those who took a placebo.
But just as with other arms of the WHI, the memory study enrolled women who were well past menopause when they started taking hormones. The subjects were aged 65 to 79. Many experts now believe there is a critical period of about 10 years after menopause when estrogen can protect women's brains, while beginning to take hormones later can be harmful. (That same critical period seems to exist for heart attack and stroke as well; women in the main WHI who started estrogen within 10 years of menopause had a decreased risk of heart attack and of death in general while women who started at older ages saw an increased risk.)
In addition, the WHIMS trial used Premarin, conjugated equine estrogen, which some experts say doesn't act on the brain as well as 17-beta estradiol. WHIMS also used a synthetic progestin that has been shown to negate some of the effects of estrogen. (Indeed, the WHIMS group that was given estrogen alone showed no increase for either Alzheimer's disease or mild cognitive impairment.) Finally, the trial used a measure of cognitive function known as the "modified mini-mental state examination" that isn't sensitive enough to assess any beneficial effects that estrogen might have had on verbal or working memory.
Many experts think the WHIMS findings needlessly frightened some women away from estrogen who might have benefited from it. Some who found the symptoms so unpleasant they've resumed. Says Dr. Devi "They say they can live with a possible future risk but that acting like an idiot today is a real problem."
There are still many unanswered questions -- including how long women should stay on estrogen. One study found that taking it for two to three years still provided protection for brain function 15 years later. Indeed, not all women suffer memory loss or fuzzy thinking at menopause, just like post-partum depression and pre-menstrual syndrome don't affect all women. "Some women are very sensitive to this decrease and some aren't," says Dr. Sherwin.
For women who are sensitive, HRT can be a lifeline. Lupe Iniguez, a tax attorney in Phoenix and mother of four found her estrogen levels so depleted in 2002 that she says "I couldn't think. I couldn't remember names of clients. I couldn't focus on documents. I resigned from every board and started to make arrangements to retire on disability." But after Dr. Vliet put her on an estradiol patch, Ms. Iniguez says, "I'm practicing full throttle again. I got my life back."
Source
Gene therapy advancing
A new way of turning genes on and off, pioneered by a Nobel prize-winning British scientist, is promising to transform treatment of conditions such as HIV/Aids, heart disease and diabetes. The technique, devised by Sir Aaron Klug, of the Laboratory of Molecular Biology in Cambridge, allows scientists to act with unprecedented precision against genes that affect a wide range of diseases, switching them on or off permanently.
The first drugs designed to target the genes have begun clinical trials in the United States on patients with arterial disease and diabetes-induced nerve damage. A third trial, for HIV, is due to begin within months. If they are successful, scientists predict that the technique could change the way many diseases are treated, making genetic therapies a routine part of medicine for the first time. In some cases, the method will be used to switch off rogue genes that promote conditions such as heart failure or cancer. In others, it will help to activate genes that protect against nerve damage or encourage blood vessel growth.
In treating HIV, the aim is to modify T-cells from patients' immune systems so that they become immune to infection with the virus. This would leave them with some working T-cells with which to fight off other infections, which are the chief cause of Aids deaths. The technique relies on a natural process by which the activity of genes is raised or lowered by proteins called transcription factors.
In 1985 Sir Aaron discovered a new class of proteins that mimic this function and can recognise specific stretches of DNA and bind to them, boosting the activity of genes or damping them down. He named them zinc-finger proteins, after the metal that holds them together and the way in which they grasp DNA. Sangamo BioSciences, a company in California, has already developed several drugs based on the principle. A zinc-finger protein specific to a gene is loaded with an enzyme called a nuclease, which will bind to the gene and turn it on or off. Sir Aaron told The Times: "We are taking nature's own method of regulating gene activity and exploiting it for our own purposes. We can use this technique to change the function of a single gene permanently. "The beauty of zinc-finger nucleases lies in their simplicity. Where other methods are long, arduous and often messy, it is relatively easy to switch off genes using this method. The zinc-finger design allows us to target a single gene, while the nuclease disrupts the gene." Details of the technique are published today in the journal Proceedings of the National Academy of Sciences.
The most advanced of Sangamo's drugs uses a zinc-finger nuclease to treat diabetic neuropathy, a common complication of diabetes that causes nerve damage and pain. The drug binds to a gene called VEGF-A, which is known to protect the nervous system, and switches it on to prevent nerve damage. Phase 2 trials of the drug are under way. The same gene is also being targeted to treat peripheral arterial disease which causes blocked arteries in the limbs. A zinc-finger drug that has started safety trials aims to stimulate VEGF-A activity, which can promote the growth of new arteries. In the longer term, a similar approach might be used to grow new blood vessels in the heart, Sir Aaron said.
Sangamo is applying for regulatory permission to start testing a zinc-finger nuclease on HIV patients as well as developing drugs to treat glioblastoma, a type of brain cancer, and single-gene disorders such as sickle-cell anaemia.
Source
****************
Just some problems with the "Obesity" war:
1). It tries to impose behavior change on everybody -- when most of those targeted are not obese and hence have no reason to change their behaviour. It is a form of punishing the innocent and the guilty alike. (It is also typical of Leftist thinking: Scorning the individual and capable of dealing with large groups only).
2). The longevity research all leads to the conclusion that it is people of MIDDLING weight who live longest -- not slim people. So the "epidemic" of obesity is in fact largely an "epidemic" of living longer.
3). It is total calorie intake that makes you fat -- not where you get your calories. Policies that attack only the source of the calories (e.g. "junk food") without addressing total calorie intake are hence pissing into the wind. People involuntarily deprived of their preferred calorie intake from one source are highly likely to seek and find their calories elsewhere.
4). So-called junk food is perfectly nutritious. A big Mac meal comprises meat, bread, salad and potatoes -- which is a mainstream Western diet. If that is bad then we are all in big trouble.
5). Food warriors demonize salt and fat. But we need a daily salt intake to counter salt-loss through perspiration and the research shows that people on salt-restricted diets die SOONER. And Eskimos eat huge amounts of fat with no apparent ill-effects. And the average home-cooked roast dinner has LOTS of fat. Will we ban roast dinners?
6). The foods restricted are often no more calorific than those permitted -- such as milk and fruit-juice drinks.
7). Tendency to weight is mostly genetic and is therefore not readily susceptible to voluntary behaviour change.
8). And when are we going to ban cheese? Cheese is a concentrated calorie bomb and has lots of that wicked animal fat in it too. Wouldn't we all be better off without it? And what about butter and margarine? They are just about pure fat. Surely they should be treated as contraband in kids' lunchboxes! [/sarcasm].
9). And how odd it is that we never hear of the huge American study which showed that women who eat lots of veggies have an INCREASED risk of stomach cancer? So the official recommendation to eat five lots of veggies every day might just be creating lots of cancer for the future! It's as plausible (i.e. not very) as all the other dietary "wisdom" we read about fat etc.
10). And will "this generation of Western children be the first in history to lead shorter lives than their parents did"? This is another anti-fat scare that emanates from a much-cited editorial in a prominent medical journal that said so. Yet this editorial offered no statistical basis for its opinion -- an opinion that flies directly in the face of the available evidence.
Even statistical correlations far stronger than anything found in medical research may disappear if more data is used. A remarkable example from Sociology:"The modern literature on hate crimes began with a remarkable 1933 book by Arthur Raper titled The Tragedy of Lynching. Raper assembled data on the number of lynchings each year in the South and on the price of an acre's yield of cotton. He calculated the correlation coefficient between the two series at -0.532. In other words, when the economy was doing well, the number of lynchings was lower.... In 2001, Donald Green, Laurence McFalls, and Jennifer Smith published a paper that demolished the alleged connection between economic conditions and lynchings in Raper's data. Raper had the misfortune of stopping his analysis in 1929. After the Great Depression hit, the price of cotton plummeted and economic conditions deteriorated, yet lynchings continued to fall. The correlation disappeared altogether when more years of data were added."So we must be sure to base our conclusions on ALL the data. But in medical research, data selectivity and the "overlooking" of discordant research findings is epidemic.
"What we should be doing is monitoring children from birth so we can detect any deviations from the norm at an early stage and action can be taken". Who said that? Joe Stalin? Adolf Hitler? Orwell's "Big Brother"? The Spanish Inquisition? Generalissimo Francisco Franco Bahamonde? None of those. It was Dr Colin Waine, chairman of Britain's National Obesity Forum. What a fine fellow!
*********************
19 March, 2008
'Cancer chemical' in soy sauce
What utter nonsense! The Japanese drink gallons of the stuff (Go Kikkoman!) and are exceptionally long-lived
AUSTRALIANS should try to limit their exposure to a "probably" cancer-causing chemical found in many common foods including soy sauce, the food regulator has urged. Food Standards Australia New Zealand said ethyl carbamate (EC) can occur naturally in foods including breads, yoghurt and alcohol that undergo fermentation during processing or storage.
The International Agency for Research on Cancer last year upgraded the risk of EC from "possibly'' carcinogenic to humans to "probably'' carcinogenic. "This knowledge suggests that limiting the consumption of some foods and responsible drinking will reduce EC intake, which would appear advisable in the light of emerging international knowledge about the chemical,'' FSANZ said today.
But the regulator said its own studies on the chemical showed it was not as great problem in Australia as some other countries. The agency last year tested food and alcohol sourced from Queensland, Victoria and Western Australia to measure the EC levels, and thereby estimate dietary exposure and potential risk to Australians' health. Among the 225 food samples tested, the chemical was found only in soy sauce. "Very low levels'' were found in 13 of the 30 types of alcoholic beverages tested, with sake, sherry and port returning the highest readings.
"When compared to overseas studies, EC levels in Australia were lower than those reported in Danish and UK surveys,'' FSANZ said. "The risk to health and safety for Australians from exposure to EC through consumption of food is therefore considered to be negligible. "The risk to health and safety for Australians from exposure to EC through alcoholic drinks, other than sake, is negligible, even for high consumers.''
But the regulator urged drinkers to stick to government guidelines on recommended alcohol consumption to minimise their risk.
Source
PESKY! Obese fare better after stroke
OBESE and overweight people are less likely to die in the five years after a stroke than are their normal weight peers, a new study shows. In the study, researchers analysed data from 21,884 stroke patients in Denmark who had their body mass index (BMI) determined. BMI is an accepted means of determining how fat or thin a person is.
The patients were placed into one of five BMI groups: underweight (BMI ( 18.5), normal weight (18.5 to 24.9), overweight (25.0 to 29.9), obese (30.0 to 34.9), and severely obese (35 and greater) and were followed for up to five years after their stroke. Compared with the normal weight individuals, the overweight, obese and severely obese subjects were 27 per cent, 16 per cent, and 16 per cent less likely, respectively, to die during follow-up, Tom Skyhoj Olsen, from Hvidovre University Hospital and colleagues found. Underweight patients, by contrast, were 63 per cent more likely to die, they report in the February 29th online issue of Neuroepidemiology.
According to the researchers, the link between obesity and poor disease outcomes, in general, is usually fuelled by the presence of other conditions. Obese people who are otherwise healthy may fare just as well as, or perhaps in the case of stroke, better than their lean counterparts, they conclude.
Source
****************
Just some problems with the "Obesity" war:
1). It tries to impose behavior change on everybody -- when most of those targeted are not obese and hence have no reason to change their behaviour. It is a form of punishing the innocent and the guilty alike. (It is also typical of Leftist thinking: Scorning the individual and capable of dealing with large groups only).
2). The longevity research all leads to the conclusion that it is people of MIDDLING weight who live longest -- not slim people. So the "epidemic" of obesity is in fact largely an "epidemic" of living longer.
3). It is total calorie intake that makes you fat -- not where you get your calories. Policies that attack only the source of the calories (e.g. "junk food") without addressing total calorie intake are hence pissing into the wind. People involuntarily deprived of their preferred calorie intake from one source are highly likely to seek and find their calories elsewhere.
4). So-called junk food is perfectly nutritious. A big Mac meal comprises meat, bread, salad and potatoes -- which is a mainstream Western diet. If that is bad then we are all in big trouble.
5). Food warriors demonize salt and fat. But we need a daily salt intake to counter salt-loss through perspiration and the research shows that people on salt-restricted diets die SOONER. And Eskimos eat huge amounts of fat with no apparent ill-effects. And the average home-cooked roast dinner has LOTS of fat. Will we ban roast dinners?
6). The foods restricted are often no more calorific than those permitted -- such as milk and fruit-juice drinks.
7). Tendency to weight is mostly genetic and is therefore not readily susceptible to voluntary behaviour change.
8). And when are we going to ban cheese? Cheese is a concentrated calorie bomb and has lots of that wicked animal fat in it too. Wouldn't we all be better off without it? And what about butter and margarine? They are just about pure fat. Surely they should be treated as contraband in kids' lunchboxes! [/sarcasm].
9). And how odd it is that we never hear of the huge American study which showed that women who eat lots of veggies have an INCREASED risk of stomach cancer? So the official recommendation to eat five lots of veggies every day might just be creating lots of cancer for the future! It's as plausible (i.e. not very) as all the other dietary "wisdom" we read about fat etc.
10). And will "this generation of Western children be the first in history to lead shorter lives than their parents did"? This is another anti-fat scare that emanates from a much-cited editorial in a prominent medical journal that said so. Yet this editorial offered no statistical basis for its opinion -- an opinion that flies directly in the face of the available evidence.
Even statistical correlations far stronger than anything found in medical research may disappear if more data is used. A remarkable example from Sociology:"The modern literature on hate crimes began with a remarkable 1933 book by Arthur Raper titled The Tragedy of Lynching. Raper assembled data on the number of lynchings each year in the South and on the price of an acre's yield of cotton. He calculated the correlation coefficient between the two series at -0.532. In other words, when the economy was doing well, the number of lynchings was lower.... In 2001, Donald Green, Laurence McFalls, and Jennifer Smith published a paper that demolished the alleged connection between economic conditions and lynchings in Raper's data. Raper had the misfortune of stopping his analysis in 1929. After the Great Depression hit, the price of cotton plummeted and economic conditions deteriorated, yet lynchings continued to fall. The correlation disappeared altogether when more years of data were added."So we must be sure to base our conclusions on ALL the data. But in medical research, data selectivity and the "overlooking" of discordant research findings is epidemic.
"What we should be doing is monitoring children from birth so we can detect any deviations from the norm at an early stage and action can be taken". Who said that? Joe Stalin? Adolf Hitler? Orwell's "Big Brother"? The Spanish Inquisition? Generalissimo Francisco Franco Bahamonde? None of those. It was Dr Colin Waine, chairman of Britain's National Obesity Forum. What a fine fellow!
*********************
18 March, 2008
Three new obesity genes discovered
Shhhh!
Three new genes that may be involved in obesity have been discovered with a new method for investigating the genetic origins of ill-health
In standard genetic studies, researchers compare the genomes of people with a medical condition and control subjects who are free from it, in search of the DNA markers that are more common in one group or the other. But in the new approach, scientists from the United States looked first at the fat and liver tissue of obese mice. By comparing their gene expression profiles with those of normal mice, they were able to identify three genes, called Lpl, Lactb and Ppml1 that appear to control weight gain.
Using the technique, the US team – led by Eric Schadt, of Rosetta Pharmaceuticals in Seattle – was also able to discover how the genes are switched on and off. The genes were found to promote inflammation in mice which in turn encouraged obesity. If these genes have similar effects in humans, it would add to the number of genes known to affect obesity. Last year a British team discovered the first gene to be reliably associated with obesity, called FTO. The research is published in the journal Nature.
Source
Hope for blindness prevetion?
A protein found in blood cells could be the key to treating or preventing two of the commonest causes of blindness, scientists in the United States believe. In mice that simulate the processes of age-related macular degeneration (AMD) and diabetic retinopathy, damage was prevented by drugs that activate a protein called Robo4, they report in Nature Medicine. The protein stopped the growth of abnormal blood vessels and stabilised existing ones, according to Professor Dean Li and colleagues from the University of Utah in Salt Lake City.
Abnormal blood vessel growth and leakage are two primary factors in AMD and diabetic retinopathy. “Many diseases are caused by injury or inflammation destabilising blood vessels and causing them to leak fluid into adjacent tissues” Professor Li said. “We found a natural pathway – the Robo4 pathway – that counter-attacks by stabilising blood vessels.”
New treatments are needed for both conditions. AMD is the commonest cause of loss of sight in the elderly and diabetic retinopathy is the commonest cause in people of working age. Treatments for one form of AMD do exist, but the best drugs are extremely expensive and at best slow down the disease. Many patients with AMD have been denied treatment with Lucentis on the NHS, at least until they have lost the sight of one eye.
The implications of the finding may go even farther because there are other diseases, such as severe acute respiratory syndrome, in which blood vessel stability is lost, allowing fluids to leak into the lungs. Tumours hijack blood vessel growth to feed on nutrients. Although this study did not prove Robo4 would treat those diseases, Professor Li believes it merits investigation.
Scientists from the University of Bristol said last week that they were ready to launch clinical trials of a drug to treat AMD and diabetic retinopathy. Professor Dave Bates and Dr Steve Harper have identified a naturally occurring form of vascular endothelial growth factor (VEGF) that inhibits the formation of new blood vessels. Professor Bates said: “We discovered the potential of VEGF165b in 2001 and have spent the last six years proving its efficacy. We plan to demonstrate clinical proof of concept of the drug in diabetic retinopathy and wet AMD patients by mid2009 so this is a very exciting time for us.” The drug technology, which has been developed with the help of the charity Fight for Sight, is being licensed to a biopharmaceutical company, PhiloGene Inc.
Source
****************
Just some problems with the "Obesity" war:
1). It tries to impose behavior change on everybody -- when most of those targeted are not obese and hence have no reason to change their behaviour. It is a form of punishing the innocent and the guilty alike. (It is also typical of Leftist thinking: Scorning the individual and capable of dealing with large groups only).
2). The longevity research all leads to the conclusion that it is people of MIDDLING weight who live longest -- not slim people. So the "epidemic" of obesity is in fact largely an "epidemic" of living longer.
3). It is total calorie intake that makes you fat -- not where you get your calories. Policies that attack only the source of the calories (e.g. "junk food") without addressing total calorie intake are hence pissing into the wind. People involuntarily deprived of their preferred calorie intake from one source are highly likely to seek and find their calories elsewhere.
4). So-called junk food is perfectly nutritious. A big Mac meal comprises meat, bread, salad and potatoes -- which is a mainstream Western diet. If that is bad then we are all in big trouble.
5). Food warriors demonize salt and fat. But we need a daily salt intake to counter salt-loss through perspiration and the research shows that people on salt-restricted diets die SOONER. And Eskimos eat huge amounts of fat with no apparent ill-effects. And the average home-cooked roast dinner has LOTS of fat. Will we ban roast dinners?
6). The foods restricted are often no more calorific than those permitted -- such as milk and fruit-juice drinks.
7). Tendency to weight is mostly genetic and is therefore not readily susceptible to voluntary behaviour change.
8). And when are we going to ban cheese? Cheese is a concentrated calorie bomb and has lots of that wicked animal fat in it too. Wouldn't we all be better off without it? And what about butter and margarine? They are just about pure fat. Surely they should be treated as contraband in kids' lunchboxes! [/sarcasm].
9). And how odd it is that we never hear of the huge American study which showed that women who eat lots of veggies have an INCREASED risk of stomach cancer? So the official recommendation to eat five lots of veggies every day might just be creating lots of cancer for the future! It's as plausible (i.e. not very) as all the other dietary "wisdom" we read about fat etc.
10). And will "this generation of Western children be the first in history to lead shorter lives than their parents did"? This is another anti-fat scare that emanates from a much-cited editorial in a prominent medical journal that said so. Yet this editorial offered no statistical basis for its opinion -- an opinion that flies directly in the face of the available evidence.
Even statistical correlations far stronger than anything found in medical research may disappear if more data is used. A remarkable example from Sociology:"The modern literature on hate crimes began with a remarkable 1933 book by Arthur Raper titled The Tragedy of Lynching. Raper assembled data on the number of lynchings each year in the South and on the price of an acre's yield of cotton. He calculated the correlation coefficient between the two series at -0.532. In other words, when the economy was doing well, the number of lynchings was lower.... In 2001, Donald Green, Laurence McFalls, and Jennifer Smith published a paper that demolished the alleged connection between economic conditions and lynchings in Raper's data. Raper had the misfortune of stopping his analysis in 1929. After the Great Depression hit, the price of cotton plummeted and economic conditions deteriorated, yet lynchings continued to fall. The correlation disappeared altogether when more years of data were added."So we must be sure to base our conclusions on ALL the data. But in medical research, data selectivity and the "overlooking" of discordant research findings is epidemic.
"What we should be doing is monitoring children from birth so we can detect any deviations from the norm at an early stage and action can be taken". Who said that? Joe Stalin? Adolf Hitler? Orwell's "Big Brother"? The Spanish Inquisition? Generalissimo Francisco Franco Bahamonde? None of those. It was Dr Colin Waine, chairman of Britain's National Obesity Forum. What a fine fellow!
*********************
17 March, 2008
New hope in fight against Alzheimer's
AUSTRALIAN researchers have discovered a drug that could delay the onset of Alzheimer's disease and improve quality of life for sufferers. A trial of 78 people conducted in Sydney, Melbourne and Sweden showed patients who took the drug for 12 weeks had a significant improvement in their ability to plan and carry out everyday activities. Professor Colin Masters, from the Mental Health Research Institute of Victoria at the University of Melbourne, said the drug could be the first to slow or reverse the early effects of Alzheimer's disease. "Disease modification, where you modify or slow down the rate of decline, is the holy grail because you can potentially delay the onset of the disease if you get in early," he said.
Dementia affects 220,000 Australians. That figure is expected to rise to 731,000 by 2050. Alzheimer's Australia executive director Glenn Rees said scientific modelling showed the ability to delay the progression of dementia by five years would halve the number of people with the disease by 2040. He said current medications could be used to treat the symptoms of dementia, such as memory loss, but they did not slow or stop the progression of the disease.
A survey of 1380 people released last month by Alzheimer's Australia and drug company Pfizer found three-quarters of those would take a test predicting their likelihood of developing the disease, if it was available. Mr Rees said a predictive test would only be useful if medication was available to treat those at risk.
The experimental drug, PBT2, reduced the amount of a protein associated with Alzheimer's in the cerebrospinal fluid, compared to the placebo. Melbourne University spin-off company Prana Biotechnology plans a larger clinical trial.
Israeli researchers last week said memory loss could be slowed significantly in mice by one of the 400 chemicals present in marijuana, called cannabidiol, which could have ramifications for Alzheimer's sufferers.
Source
Blood clot pill approved in Britain
A daily pill that could help to prevent tens of thousands of deaths due to blood clots will be available to hospitals within weeks. The condition, venous thrombo-embolism (VTE), causes one in ten fatalities in hospital and kills at least 25,000 people in England every year, more than 20 times the number of deaths attributed to the superbug MRSA.
Pradaxa, the first new blood-thinning treatment in more than 50 years, is set to receive its licence next month. It will be used initially after hip and knee replacement surgery when the risk of blood clotting is high. But doctors hope that the anticoagulant pill could also be used to treat thousands of other patients at risk from heart conditions and strokes.
As many as half of all patients going into hospital risk developing VTE, which occurs when part of a deep-vein thrombosis or blood clot migrates to the lungs, heart or brain, with potentially deadly consequences. Such clotting is common after surgery, especially in the elderly, the overweight or those confined to bed for more than three days.
Last year the National Institute for Health and Clinical Excellence (NICE) issued guidelines recommending that all patients should be assessed on admission to hospital for their risk of developing VTE but an audit by the all-party parliamentary thrombosis group in November found that less than a third of hospitals were doing so. Of those who were screened, only half the patients deemed at risk were receiving preventive treatment, a study published in The Lancet last month suggested.
A report by Sir Liam Donaldson, the Chief Medical Officer, admitted that "there was no systematic approach to identifying and treating those patients at risk from blood clots in hospitals and that there was significant room for improvement". At present, many hospital patients at risk of blood clots are given warfarin, which was licensed in the 1950s. Warfarin is effective but can trigger excessive internal bleeding. An alternative drug, heparin, involves a lengthy course of injections.
Preliminary results from a trial involving 34,000 patients suggest that Pradaxa is as effective in preventing clotting as existing treatments but it should be cheaper and easier to take. It works by reversing and inhibiting the effects of thrombin, a protein that allows clots to form after surgery.
Produced by the German company Boehringer Ingelheim, the drug is being evaluated by NICE and if approved it could be available to NHS patients within weeks. Another anticoagulant, Xarelto, is in development by Bayer, with preliminary results suggesting that it could be even more effective than Pradaxa.
Simon Frostick, a specialist in orthopaedics at the University of Liverpool, said: "These new drugs will revolutionise the way we prevent and treat blood clots. "Given the new trend for shorter hospital stays following joint replacement surgery, it is becoming increasingly important to have anticoagulant treatments available which are well tolerated and easy to use."
Beverley Hunt, medical director of the UK thrombosis charity Lifeblood, said: "The number of deaths from VTE is nothing short of a public health emergency. "The development of new drugs to treat this problem is terribly exciting. The potential benefit to the NHS is enormous."
Between 1995 and 2003, the NHS Litigation Authority handled more than 450 claims of negligence after patients developed VTE in hospital. It paid out almost 19 million pounds in compensation to sufferers or their bereaved families.
Professor Frostick added: "If these drugs reduce the number of deaths, the requirement for injections and community nurses, as well as other burdens - and if the proper sums are done - they should work out to be cost-effective for the NHS."
Source
****************
Just some problems with the "Obesity" war:
1). It tries to impose behavior change on everybody -- when most of those targeted are not obese and hence have no reason to change their behaviour. It is a form of punishing the innocent and the guilty alike. (It is also typical of Leftist thinking: Scorning the individual and capable of dealing with large groups only).
2). The longevity research all leads to the conclusion that it is people of MIDDLING weight who live longest -- not slim people. So the "epidemic" of obesity is in fact largely an "epidemic" of living longer.
3). It is total calorie intake that makes you fat -- not where you get your calories. Policies that attack only the source of the calories (e.g. "junk food") without addressing total calorie intake are hence pissing into the wind. People involuntarily deprived of their preferred calorie intake from one source are highly likely to seek and find their calories elsewhere.
4). So-called junk food is perfectly nutritious. A big Mac meal comprises meat, bread, salad and potatoes -- which is a mainstream Western diet. If that is bad then we are all in big trouble.
5). Food warriors demonize salt and fat. But we need a daily salt intake to counter salt-loss through perspiration and the research shows that people on salt-restricted diets die SOONER. And Eskimos eat huge amounts of fat with no apparent ill-effects. And the average home-cooked roast dinner has LOTS of fat. Will we ban roast dinners?
6). The foods restricted are often no more calorific than those permitted -- such as milk and fruit-juice drinks.
7). Tendency to weight is mostly genetic and is therefore not readily susceptible to voluntary behaviour change.
8). And when are we going to ban cheese? Cheese is a concentrated calorie bomb and has lots of that wicked animal fat in it too. Wouldn't we all be better off without it? And what about butter and margarine? They are just about pure fat. Surely they should be treated as contraband in kids' lunchboxes! [/sarcasm].
9). And how odd it is that we never hear of the huge American study which showed that women who eat lots of veggies have an INCREASED risk of stomach cancer? So the official recommendation to eat five lots of veggies every day might just be creating lots of cancer for the future! It's as plausible (i.e. not very) as all the other dietary "wisdom" we read about fat etc.
10). And will "this generation of Western children be the first in history to lead shorter lives than their parents did"? This is another anti-fat scare that emanates from a much-cited editorial in a prominent medical journal that said so. Yet this editorial offered no statistical basis for its opinion -- an opinion that flies directly in the face of the available evidence.
Even statistical correlations far stronger than anything found in medical research may disappear if more data is used. A remarkable example from Sociology:"The modern literature on hate crimes began with a remarkable 1933 book by Arthur Raper titled The Tragedy of Lynching. Raper assembled data on the number of lynchings each year in the South and on the price of an acre's yield of cotton. He calculated the correlation coefficient between the two series at -0.532. In other words, when the economy was doing well, the number of lynchings was lower.... In 2001, Donald Green, Laurence McFalls, and Jennifer Smith published a paper that demolished the alleged connection between economic conditions and lynchings in Raper's data. Raper had the misfortune of stopping his analysis in 1929. After the Great Depression hit, the price of cotton plummeted and economic conditions deteriorated, yet lynchings continued to fall. The correlation disappeared altogether when more years of data were added."So we must be sure to base our conclusions on ALL the data. But in medical research, data selectivity and the "overlooking" of discordant research findings is epidemic.
"What we should be doing is monitoring children from birth so we can detect any deviations from the norm at an early stage and action can be taken". Who said that? Joe Stalin? Adolf Hitler? Orwell's "Big Brother"? The Spanish Inquisition? Generalissimo Francisco Franco Bahamonde? None of those. It was Dr Colin Waine, chairman of Britain's National Obesity Forum. What a fine fellow!
*********************
16 March, 2008
IS DRINKING TEA GOOD FOR YOU?
The study below says that French women who drink a lot of tea (French women drink tea??) are less likely to get clogged arteries. But is that BECAUSE of the tea or because of whatever it is that makes French women abandon coffee? No need to wonder, though. The replication study below showed differences that were not statistically significant (.08 >.05). So the initial finding looks to have been just a statistical fluke. Both the heading and the conclusions are then essentially lies. How do they get away with it?
Tea Consumption Is Inversely Associated With Carotid Plaques in Women
Stephanie Debette et al.
Abstract
Objective: The aim of this study was to assess the relationship of tea consumption with common carotid artery intima-media thickness (CCA-IMT) and carotid plaques.
Methods and Results: The study was performed on 6597 subjects aged ~ 65 years, recruited in the French population for the Three-City Study. Atherosclerotic plaques in the extracranial carotid arteries and CCA-IMT were measured using a standardized protocol. Results were tested for replication in another, younger, French population sample (EVA-Study, 1123 subjects). In the Three-City Study, increasing daily tea consumption was associated with a lower prevalence of carotid plaques in women: 44.0%, 42.5%, and 33.7% in women drinking no tea, 1 to 2 cups/d, and ~3 cups/d (P=0.0001). This association was independent of age, center, major vascular risk factors, educational level, and dietary habits (adjOR=0.68[95%CI:0.54 to 0.86] for women drinking cups/d compared with none). There was no association of tea consumption with carotid plaques in men, or CCA-IMT in both genders. In the EVA-Study, carotid plaque frequency was 18.8%, 18.5%, and 8.9% in women drinking no tea, 1 to 2 cups/d, and ~3 cups/d (P=0.08).
Conclusion— In a large sample of elderly community subjects we showed for the first time that carotid plaques were less frequent with increasing tea consumption in women.
Our aim was to assess the relationship of tea consumption with common carotid artery intima-media thickness and carotid plaques in a large population-based sample of elderly subjects. Increasing daily tea consumption was associated with a lower prevalence of carotid plaques in women, independently of vascular risk factors and dietary habits.
Arteriosclerosis, Thrombosis, and Vascular Biology. 2008;28:353.
Pepper drugs fight memory as well as pain
A new class of painkillers derived from chilli peppers may interfere with brain functions such as learning and memory, a study suggests. Drug companies have been testing medicines based on the action of capsaicin, the fiery compound in chillis, which can temporarily desensitise the body's pain sensors. The drugs are designed to be targeted against only the nerves involved in sending pain signals to the brain but experiments on rats have suggested that the painkilling action might have a knock-on effect.
US researchers writing in the journal Neuron say that the drugs' target, a brain receptor known as TRPV1, regulates processes central to mood and memory as well as pain. The findings may also help to explain the potentially suicidal side-effects of the antiobesity drug Acomplia, which has been taken by more than 40,000 Britons. The researchers say that this could be linked to the drug "antagonising" the TRPV1 receptor.
Source
****************
Just some problems with the "Obesity" war:
1). It tries to impose behavior change on everybody -- when most of those targeted are not obese and hence have no reason to change their behaviour. It is a form of punishing the innocent and the guilty alike. (It is also typical of Leftist thinking: Scorning the individual and capable of dealing with large groups only).
2). The longevity research all leads to the conclusion that it is people of MIDDLING weight who live longest -- not slim people. So the "epidemic" of obesity is in fact largely an "epidemic" of living longer.
3). It is total calorie intake that makes you fat -- not where you get your calories. Policies that attack only the source of the calories (e.g. "junk food") without addressing total calorie intake are hence pissing into the wind. People involuntarily deprived of their preferred calorie intake from one source are highly likely to seek and find their calories elsewhere.
4). So-called junk food is perfectly nutritious. A big Mac meal comprises meat, bread, salad and potatoes -- which is a mainstream Western diet. If that is bad then we are all in big trouble.
5). Food warriors demonize salt and fat. But we need a daily salt intake to counter salt-loss through perspiration and the research shows that people on salt-restricted diets die SOONER. And Eskimos eat huge amounts of fat with no apparent ill-effects. And the average home-cooked roast dinner has LOTS of fat. Will we ban roast dinners?
6). The foods restricted are often no more calorific than those permitted -- such as milk and fruit-juice drinks.
7). Tendency to weight is mostly genetic and is therefore not readily susceptible to voluntary behaviour change.
8). And when are we going to ban cheese? Cheese is a concentrated calorie bomb and has lots of that wicked animal fat in it too. Wouldn't we all be better off without it? And what about butter and margarine? They are just about pure fat. Surely they should be treated as contraband in kids' lunchboxes! [/sarcasm].
9). And how odd it is that we never hear of the huge American study which showed that women who eat lots of veggies have an INCREASED risk of stomach cancer? So the official recommendation to eat five lots of veggies every day might just be creating lots of cancer for the future! It's as plausible (i.e. not very) as all the other dietary "wisdom" we read about fat etc.
10). And will "this generation of Western children be the first in history to lead shorter lives than their parents did"? This is another anti-fat scare that emanates from a much-cited editorial in a prominent medical journal that said so. Yet this editorial offered no statistical basis for its opinion -- an opinion that flies directly in the face of the available evidence.
Even statistical correlations far stronger than anything found in medical research may disappear if more data is used. A remarkable example from Sociology:"The modern literature on hate crimes began with a remarkable 1933 book by Arthur Raper titled The Tragedy of Lynching. Raper assembled data on the number of lynchings each year in the South and on the price of an acre's yield of cotton. He calculated the correlation coefficient between the two series at -0.532. In other words, when the economy was doing well, the number of lynchings was lower.... In 2001, Donald Green, Laurence McFalls, and Jennifer Smith published a paper that demolished the alleged connection between economic conditions and lynchings in Raper's data. Raper had the misfortune of stopping his analysis in 1929. After the Great Depression hit, the price of cotton plummeted and economic conditions deteriorated, yet lynchings continued to fall. The correlation disappeared altogether when more years of data were added."So we must be sure to base our conclusions on ALL the data. But in medical research, data selectivity and the "overlooking" of discordant research findings is epidemic.
"What we should be doing is monitoring children from birth so we can detect any deviations from the norm at an early stage and action can be taken". Who said that? Joe Stalin? Adolf Hitler? Orwell's "Big Brother"? The Spanish Inquisition? Generalissimo Francisco Franco Bahamonde? None of those. It was Dr Colin Waine, chairman of Britain's National Obesity Forum. What a fine fellow!
*********************
15 March, 2008
Food Fascism gets 8th-grader punished
What could be more normal than a kid eating candy? But the Fascists are determined to stop it
Contraband candy has led to big trouble for an eighth-grade honors student in Connecticut. Michael Sheridan was stripped of his title as class vice president, barred from attending an honors student dinner and suspended for a day after buying a bag of Skittles from a classmate. School spokeswoman Catherine Sullivan-DeCarlo says the New Haven school system banned candy sales in 2003 as part of a districtwide school wellness policy.
Michael's suspension has been reduced from three days to one, but he has not been reinstated as class vice president. He says he didn't realize his candy purchase was against the rules, but he did notice the student selling the Skittles on Feb. 26 was being secretive.
Source
Vaccines Are Safe
Over the past decade, the public has been presented with a large amount of information about the safety of vaccines. Among the reasons for this interest is the widespread success of routine, universal immunization of infants and children, beginning in the 1940s. Unfortunately, along with reasonable information comes erroneous information, and the safety and effectiveness of vaccines has been questioned. Make no mistake: Many dangerous, life-threatening diseases have been wiped out because of vaccines. Immunization was the greatest public health achievement in the U.S. in the 20th century.
The list of licensed and recommended vaccines has been growing, and not just for infants and children. There are now schedules from professional societies, such as the American Academy of Family Physicians (AAFP) and the American College of Obstetricians and Gynecologists (ACOG) and public agencies (e.g., the U.S. Centers for Disease Control and Prevention) that indicate what vaccines should be given for adolescents and adults, and when. There are specific vulnerable populations.
The considerable focus on vaccines, and their safety, in our information-overloaded society is not surprising, with a surplus of articles in magazines, books, parenting guides, and on the Internet, and stories on radio and television. While these occasionally highlight the benefits of immunization - "No One Got Sick or Died from a Vaccine-Preventable Disease Today" - is not a very exciting story.
More often, the emphasis is on speculation that a vaccine caused a health problem. Further, the widespread availability of litigation and liberal tort in the U.S. has encouraged lawsuits claiming harm from vaccines. Finally, it's human nature to assume cause-and-effect when something bad happens, so a vaccination is an attractive target when administered before the onset of a medical condition. Unfortunately, most of the public receives a lot of health information from these lay sources, rather than their physicians. Professional knowledge of immunization is grounded in science - microbiology, immunology, epidemiology, and statistics.
Vaccines are licensed by the U.S. Federal Drug Administration (FDA) only when proven to be safe and effective. Recommendations for use are promulgated by committees of scientific experts composed of academics, clinicians and other caregivers that are passionately devoted to our citizens' health and safety. The committees' conclusions, and the rationale for them, are shared with practicing physicians, who are the most reliable source of information for patients. This process is the foundation that leads to the conclusions that licensed vaccines are safe, and fears that vaccines are harmful are unfounded.
Nevertheless, to address these unfounded fears, groups of scientific experts have undertaken investigations to determine possible relationships between vaccines and autism, asthma, diabetes, multiple sclerosis, SIDS, and other diseases, and to ansrwer questions that are posed to them:
Does hepatitis B vaccine cause SIDS? Looking at the numbers of doses administered of the former and cases of the latter, one would conclude the opposite, that hepatitis B vaccine prevents SIDS, since 90 percent of U.S. children have received hepatitis B vaccine, and SIDS cases have dropped dramatically in the past decade (probably due to the AAP recommendation that infants sleep on their backs).
Does the MMR vaccine cause autism? This question received extraordinary attention after it was raised in an article in The Lancet, in 1998, by Drs. Wakefield and colleagues. The co-authors and The Lancet have since retracted the article and its conclusions, and Dr. Wakefield is currently on trial in the U.K. for conflict of interest at the time of its publication. (He was on retainer from lawyers suing for vaccine damages.)
More importantly, an Institute of Medicine (IOM) expert panel evaluated the issue, and concluded that the evidence favored rejection of a connection between autism and MMR vaccine. Fourteen epidemiologic studies have been performed, all demonstrating the absence of a relationship between increased rates of autism and frequency of use of MMR vaccine.
It is unfortunate that the speculation of a relationship between MMR vaccine and autism has resulted in the occurrence of vaccine-preventable diseases (especially measles) in children whose parents refused to allow them to receive the vaccine, and has diverted attention from research into the causes of autism, which has been shown to have prenatal origins.
Is thimerosal a cause of neurologic abnormalities, including autism? The preservative thimerosal, consisting of ethyl mercury, was used in multi-dose vaccine vials. At present, most infancy and childhood vaccines are supplied in single-dose vials, and all such routine vaccines are thimerosal-free. Studies to answer this question, including five epidemiologic surveys, came to the same conclusion as the MMR vaccine autism analyses, that there is absence of a relationship. A pivotal study at the University of Rochester quantifying thimerosal in childhood vaccines stated administration of vaccines containing thimerosal does not seem to raise blood concentrations of mercury above safe values in infants. In short, no studies have established a causal link between vaccines and these diseases.
Many of us recall that only two generations ago we had schoolmates who limped or had withered arms, due to the paralytic polio that infected them. That disease has been eradicated in the U.S. because of the universal use of polio vaccine. During my training, I cared for children made deaf from measles, infants blind and retarded from rubella, and those who died from bacteria like pneumococcus and meningococcus. With vaccination, those conditions no longer occur.
As a physician in my early years of practice, the threat of infection with bacteria called Haemophilus influenza type B (Hib) loomed large for my patients and their families; the outcomes of brain damage or death being distinct possibilities. A vaccine was invented, adopted as policy, and given to U.S. infants and children. I'm pleased to say I no longer worry about Hib infection.
Despite scientific proof and a long track record of vaccine safety, we see public policy based on junk beliefs, misinformation, fear, and mass hysteria. In 2006, a number of legislative bodies passed, and executives signed, bills prohibiting use of vaccines containing thimerosal.
From a practical perspective, these restrictions mean little, since all but a few influenza vaccines do not contain thimerosal. But such policies send a bad message: The vaccines that have virtually eradicated many diseases, constituting one of the greatest public health accomplishments of the past century, are dangerous. Further, these policies denigrate our informed medical and scientific communities. This is a disservice to our citizens, and endangers us all.
Source
****************
Just some problems with the "Obesity" war:
1). It tries to impose behavior change on everybody -- when most of those targeted are not obese and hence have no reason to change their behaviour. It is a form of punishing the innocent and the guilty alike. (It is also typical of Leftist thinking: Scorning the individual and capable of dealing with large groups only).
2). The longevity research all leads to the conclusion that it is people of MIDDLING weight who live longest -- not slim people. So the "epidemic" of obesity is in fact largely an "epidemic" of living longer.
3). It is total calorie intake that makes you fat -- not where you get your calories. Policies that attack only the source of the calories (e.g. "junk food") without addressing total calorie intake are hence pissing into the wind. People involuntarily deprived of their preferred calorie intake from one source are highly likely to seek and find their calories elsewhere.
4). So-called junk food is perfectly nutritious. A big Mac meal comprises meat, bread, salad and potatoes -- which is a mainstream Western diet. If that is bad then we are all in big trouble.
5). Food warriors demonize salt and fat. But we need a daily salt intake to counter salt-loss through perspiration and the research shows that people on salt-restricted diets die SOONER. And Eskimos eat huge amounts of fat with no apparent ill-effects. And the average home-cooked roast dinner has LOTS of fat. Will we ban roast dinners?
6). The foods restricted are often no more calorific than those permitted -- such as milk and fruit-juice drinks.
7). Tendency to weight is mostly genetic and is therefore not readily susceptible to voluntary behaviour change.
8). And when are we going to ban cheese? Cheese is a concentrated calorie bomb and has lots of that wicked animal fat in it too. Wouldn't we all be better off without it? And what about butter and margarine? They are just about pure fat. Surely they should be treated as contraband in kids' lunchboxes! [/sarcasm].
9). And how odd it is that we never hear of the huge American study which showed that women who eat lots of veggies have an INCREASED risk of stomach cancer? So the official recommendation to eat five lots of veggies every day might just be creating lots of cancer for the future! It's as plausible (i.e. not very) as all the other dietary "wisdom" we read about fat etc.
10). And will "this generation of Western children be the first in history to lead shorter lives than their parents did"? This is another anti-fat scare that emanates from a much-cited editorial in a prominent medical journal that said so. Yet this editorial offered no statistical basis for its opinion -- an opinion that flies directly in the face of the available evidence.
Even statistical correlations far stronger than anything found in medical research may disappear if more data is used. A remarkable example from Sociology:"The modern literature on hate crimes began with a remarkable 1933 book by Arthur Raper titled The Tragedy of Lynching. Raper assembled data on the number of lynchings each year in the South and on the price of an acre's yield of cotton. He calculated the correlation coefficient between the two series at -0.532. In other words, when the economy was doing well, the number of lynchings was lower.... In 2001, Donald Green, Laurence McFalls, and Jennifer Smith published a paper that demolished the alleged connection between economic conditions and lynchings in Raper's data. Raper had the misfortune of stopping his analysis in 1929. After the Great Depression hit, the price of cotton plummeted and economic conditions deteriorated, yet lynchings continued to fall. The correlation disappeared altogether when more years of data were added."So we must be sure to base our conclusions on ALL the data. But in medical research, data selectivity and the "overlooking" of discordant research findings is epidemic.
"What we should be doing is monitoring children from birth so we can detect any deviations from the norm at an early stage and action can be taken". Who said that? Joe Stalin? Adolf Hitler? Orwell's "Big Brother"? The Spanish Inquisition? Generalissimo Francisco Franco Bahamonde? None of those. It was Dr Colin Waine, chairman of Britain's National Obesity Forum. What a fine fellow!
*********************
14 March, 2008
Short men 'more likely to be jealous'
This is not really news. You don't have to be Einstein to know that women prefer tall men and men prefer beautiful women. So plain women or short men are more likely to be rejected and therefore more jealous!
It does however highlight one thing that is often overlooked: That the preference for taller men tends to leave tall women rather high and dry. They find difficulty in getting men who are taller than them. So when they see a one of the rare really tall men with a short lady it does tend to get them irritated ("jealous"). They think that the short lady concerned is taking away one of their rare opportunities. How do I know that? I am tall enough to have had quite a few tall women in my life and they talk to me. And I listen!
Jealous lovers need look no further than their height if they want something to blame for their attacks of the green-eyed monster, new research shows. A study by Spanish and Dutch researchers has found that the shorter a man is the more likely he is to suffer bouts of jealousy. European men questioned by the scientists at the Universities of Groningen and Valencia said they felt most threatened by romantic rivals who were attractive, rich and strong, the New Scientist magazine reported.
Women, on the other hand, were most jealous of others' beauty and charm. They were also most prone to jealousy if they were either short or tall, with medium-height females feeling the most relaxed.
Sydney-based psychotherapist Steven Carroll said the findings, published in the US journal Evolution and Human Behaviour, made evolutionary sense. "From an Australian perspective this is quite right because studies have shown that taller men do best with the ladies," Mr Carroll said. "Young rural Australian men have been seen to worry less about the girls the taller they are and other research has shown that shorter men are more likely to provoke taller men into fights."
But Mr Carroll said when a women actually leaves her partner for another man, jealousy will appear irrespective of height. "The new man could be a midget on life support or Arnold Schwarzenegger and it really wouldn't make a difference to jealousy levels."
The European researchers say it makes sense women of average height are least jealous because, from an evolutionary perspective, they are the most fertile, in the best health, and most popular with men. Mr Carroll agreed but said height was a more complex issue among women, especially in Australia. "Yes, there's the evolutionary angle of average height but in Australia there is much more social pressure than evolutionary pressure to be supermodel tall and fit this legs-up-to-here ideal, and that plays a role too," he said.
The study surveyed 549 men and women in the Netherlands and Spain, with Mr Carroll saying it was "fascinating" the shorter and famously jealous Spaniards had collaborated with the cool and considerably taller Dutch for the research.
Source
Tell a big enough lie often enough ...
The article below is probably correct about the extent to which cholesterol can be lowered. That lower dietary cholesterol would save lives is the lie
Lowering the cholesterol of every Australian by 10 per cent would save 3000 lives a year, according to research which calls for a nationwide shift on diet and exercise. The study by Sydney researchers has found that a small, 10 per cent drop in "bad" LDL cholesterol could be achieved in just a few weeks, primarily by cutting back on saturated fats and exercising more. The shift would save 3000 people annually who would otherwise be dead from heart attack, cardiovascular disease or ischaemic stroke, the researchers at the George Institute for International Health found.
"These are quite significant findings," said Dr Rachel Huxley, the institute's director of nutrition and lifestyle. "We're not talking drugs; we're talking simple diet and exercise changes that an individual can make to lower their LDL in less than a month."
The key change would be lowering saturated fat intake, particularly full fat dairy products, convenience meals, takeaway foods, confectionary, cakes and biscuits - the biggest contributors to LDL in Australia. Statistics show about 12 per cent of energy consumed in an average Australian diet comes from saturated fats, 50 per cent above recommended levels. "If we could cut down on those food items we could make a substantial contribution to reducing the amount of saturate fats that we consume and the number of people that are dying," Dr Huxley said.
Source
****************
Just some problems with the "Obesity" war:
1). It tries to impose behavior change on everybody -- when most of those targeted are not obese and hence have no reason to change their behaviour. It is a form of punishing the innocent and the guilty alike. (It is also typical of Leftist thinking: Scorning the individual and capable of dealing with large groups only).
2). The longevity research all leads to the conclusion that it is people of MIDDLING weight who live longest -- not slim people. So the "epidemic" of obesity is in fact largely an "epidemic" of living longer.
3). It is total calorie intake that makes you fat -- not where you get your calories. Policies that attack only the source of the calories (e.g. "junk food") without addressing total calorie intake are hence pissing into the wind. People involuntarily deprived of their preferred calorie intake from one source are highly likely to seek and find their calories elsewhere.
4). So-called junk food is perfectly nutritious. A big Mac meal comprises meat, bread, salad and potatoes -- which is a mainstream Western diet. If that is bad then we are all in big trouble.
5). Food warriors demonize salt and fat. But we need a daily salt intake to counter salt-loss through perspiration and the research shows that people on salt-restricted diets die SOONER. And Eskimos eat huge amounts of fat with no apparent ill-effects. And the average home-cooked roast dinner has LOTS of fat. Will we ban roast dinners?
6). The foods restricted are often no more calorific than those permitted -- such as milk and fruit-juice drinks.
7). Tendency to weight is mostly genetic and is therefore not readily susceptible to voluntary behaviour change.
8). And when are we going to ban cheese? Cheese is a concentrated calorie bomb and has lots of that wicked animal fat in it too. Wouldn't we all be better off without it? And what about butter and margarine? They are just about pure fat. Surely they should be treated as contraband in kids' lunchboxes! [/sarcasm].
9). And how odd it is that we never hear of the huge American study which showed that women who eat lots of veggies have an INCREASED risk of stomach cancer? So the official recommendation to eat five lots of veggies every day might just be creating lots of cancer for the future! It's as plausible (i.e. not very) as all the other dietary "wisdom" we read about fat etc.
10). And will "this generation of Western children be the first in history to lead shorter lives than their parents did"? This is another anti-fat scare that emanates from a much-cited editorial in a prominent medical journal that said so. Yet this editorial offered no statistical basis for its opinion -- an opinion that flies directly in the face of the available evidence.
Even statistical correlations far stronger than anything found in medical research may disappear if more data is used. A remarkable example from Sociology:"The modern literature on hate crimes began with a remarkable 1933 book by Arthur Raper titled The Tragedy of Lynching. Raper assembled data on the number of lynchings each year in the South and on the price of an acre's yield of cotton. He calculated the correlation coefficient between the two series at -0.532. In other words, when the economy was doing well, the number of lynchings was lower.... In 2001, Donald Green, Laurence McFalls, and Jennifer Smith published a paper that demolished the alleged connection between economic conditions and lynchings in Raper's data. Raper had the misfortune of stopping his analysis in 1929. After the Great Depression hit, the price of cotton plummeted and economic conditions deteriorated, yet lynchings continued to fall. The correlation disappeared altogether when more years of data were added."So we must be sure to base our conclusions on ALL the data. But in medical research, data selectivity and the "overlooking" of discordant research findings is epidemic.
"What we should be doing is monitoring children from birth so we can detect any deviations from the norm at an early stage and action can be taken". Who said that? Joe Stalin? Adolf Hitler? Orwell's "Big Brother"? The Spanish Inquisition? Generalissimo Francisco Franco Bahamonde? None of those. It was Dr Colin Waine, chairman of Britain's National Obesity Forum. What a fine fellow!
*********************
13 March, 2008
The Obesity Police Are Coming
Lawmakers in Mississippi have proposed a bill that would revoke the business license of any restaurant that serves food to fat people, as measured by state health standards. Proponents of the paternalistic nanny-state are intent on transforming obesity into a public health issue. But obesity is a private health matter, of no legitimate concern to government.
Each individual has a right to life, which includes the right to eat as one sees fit. A rational judgment about what to eat takes into account many individual factors--nutritional needs, metabolism, genetics, medical history, and a doctor's advice--as well as the pleasure of eating and one's personal views on body shape. The fact that some people may irrationally maintain an unhealthy weight by overeating cannot justify government control over food intake.
Legitimate public health measures, such as quarantining persons with infectious diseases or outlawing disease-spreading cesspools, involve shielding innocent victims from physical force. But fat people do not emit physical forces that impede other people's freedom of action. Hence, government has no right to prevent or punish obesity.
Some say body weight is a proper subject of legislation because taxpayers bear the burden of treating obesity-related maladies. But the solution to escalating health-care costs is not to surrender control of our bodies but to question the prevailing view that government should be involved in paying for health care.
Obese individuals have the same right as anyone else to decide what to eat, and restaurant owners have a right to choose whom they will serve. The Mississippi legislative proposal is a particularly ugly, arrogant attempt to decree public ownership of human bodies. As such, it is an attack on everyone's freedom, and it should be denounced as such.
Source
Fat kid = unfit parent?
The societal panic over childhood obesity, already entrenched in the medical system and evident in the furor over school lunches, is beginning to influence custody judgments and child-welfare authorities in their decisions about fitness to parent. An Ontario family court judgment involving the Children's Aid Society recently cited obesity as a reason for removing a child from the parental home, after determining the mother was contributing to her child's weight gain and was oblivious to the required medical regime.
The details of the case are covered by a publication ban, but the theme is echoed in another case, an epic nine-year custody battle that wrapped up in a Newmarket courtroom last month, much of which centred on the comparative merits of the battling parents in adhering to a diet plan for their obese twins. The children, who were toddlers when the custody dispute began and who were 10 when it was finally resolved in favour of the mother last month, have spent most of their lives in intensive hospital-based obesity programs.
The custody dispute between their parents, Robert and Lisa, pushed the limits of the extent to which childhood obesity could be considered a result of parental neglect, with evidence in the case using language that makes poor nutritional choices seem tantamount to child abuse. The father, Robert, for example, argued that it was "manifestly obvious that the health and very lives of the children were under imminent threat due to their mother's refusal to comply with prescribed nutritional regimes and not overfeed the children," according to the judgment in the case, released on Feb. 11.
The case even drew on the evidence of a renowned childhood obesity expert, Dr. Glenn Berall, chief of pediatrics at North York General Hospital, who described himself as an "advocate for the children" and who urged the court to place the children in the direct care of the parent who had demonstrated the ability to comply with a prescribed weight-management program and to restrict access to the parent who did not reasonably comply. Elliot Birnboim, the lawyer for the mother in the dispute, said this case was the first time the issue of childhood obesity was the primary issue put forth for determining custody.
Even adoption applications are being considered in this way. Last summer, a family court judge in Kansas City deemed Gary Stocklaufer "an unfit adoptive parent" because he was grossly overweight. Weighing more than 500 pounds, he was rejected for health reasons, but was awarded custody this year after undergoing gastric bypass surgery and losing about 200 pounds.
These far-reaching measures suggest the state may increasingly seek a role in the kitchens of the nation, a reflection of cultural attitudes that put obesity beyond mere medical concern and perhaps more in line of social scourge. A recent study found that Canadian childhood obesity rates rank fifth-highest of 34 developed countries. Rates have soared in the past 30 years, from 5% to 30%, with more children reporting ailments common in obese adults, such as joint degradation, Type 2 diabetes, hypertension and respiratory illnesses.
The morality of obesity has come up in the debate over the rise in the number of patients considered "super obese," and whether the medical system or the patient should bear the cost of oversized equipment. Charlene Elliott, an assistant professor at the University of Calgary who researches obesity, was not aware of these specific cases, but said it is interesting to consider "ways in which society's attitudes on obesity play out differently depending on whether the obese individual is an adult or a child."
"If you examine both the media and societal framing of obesity, you will observe a consistent shift in terms of responsibility depending on who is obese. Adults are considered to be responsible for their own bodies [and body size] whereas children are framed as vulnerable -- 'victims' of adult decisions and, therefore, not responsible for their size," she said.
She said this attitude is why, in the context of childhood obesity, there are "all sorts of social engineering remedies playing out," such as policies intended to make the environment more healthy for children, including the lobbying to extend the ban Quebec has on television advertising to children under the age of 13 to the rest of Canada, the banning of sugary sodas in elementary schools, and the mandatory 20 minutes of physical activity in schools.
"My take on this is that obesity should be treated no differently than other cases where conditions can lead to limited fitness to parent," said Dr. Arya Sharma, chairman for obesity research and management at the University of Alberta and scientific director of the Canadian Obesity Network. "Obesity is not a moral failing or necessarily always a lifestyle problem. One has to very specifically look at the causes of obesity -- these can be varied, ranging from genetics, mental-health problems, medications and other issues that may be difficult to control. [In the case of parenting] with the exception of extreme cases, where severe obesity may result in physical limitations to actually look after the kids, in itself increased body weight does not necessarily translate into inability to parent."
Mr. Birnboim, the lawyer in the Newmarket custody dispute, said the ruling was significant because it swept aside "the prejudices about obesity" to try to consider the overall condition of the children. According to the judgment, the parents "have been in almost continuous litigation concerning the diet, health and residence" of their twins. When the children were just two years old, Dr. Berall determined the boy was morbidly obese and his sister overweight, and set them on a prescribed course that included twice-weekly weigh-ins. At one point in the long-running custody battle, he told the court "consistently, with rare exceptions, the children lost weight under the care of their father and consistently gained weight, with rare exceptions, under the care of their mother."
Robert, the father, put forth a custody plan that gave him "sole responsibility for the children's health care, for the primary reason that he could enhance and direct the children's ongoing weight-management program," the judgment said.
The mother, Lisa, argued against the father gaining full custody, saying that his approach to parenting was "his continuous attendances with the children on numerous medical reviews, weigh-ins and the administering of blood tests; combined with his continuous negative references to others and directly to the children that they are overweight, not normal and are ill and in danger of developing certain conditions or diseases."
In the end, the court determined that primary custody should go to the mother, where the children seemed most happy and well-adjusted, while conceding "the weight-management of the children was a problem that needed addressing." "There's no question that obesity has been a hot issue," Mr. Birnboim said. "Not to downplay the health issue, but we've got to push aside some of the prejudices we have about obesity. It doesn't preempt having a happy, well-adjusted child."
Source
****************
Just some problems with the "Obesity" war:
1). It tries to impose behavior change on everybody -- when most of those targeted are not obese and hence have no reason to change their behaviour. It is a form of punishing the innocent and the guilty alike. (It is also typical of Leftist thinking: Scorning the individual and capable of dealing with large groups only).
2). The longevity research all leads to the conclusion that it is people of MIDDLING weight who live longest -- not slim people. So the "epidemic" of obesity is in fact largely an "epidemic" of living longer.
3). It is total calorie intake that makes you fat -- not where you get your calories. Policies that attack only the source of the calories (e.g. "junk food") without addressing total calorie intake are hence pissing into the wind. People involuntarily deprived of their preferred calorie intake from one source are highly likely to seek and find their calories elsewhere.
4). So-called junk food is perfectly nutritious. A big Mac meal comprises meat, bread, salad and potatoes -- which is a mainstream Western diet. If that is bad then we are all in big trouble.
5). Food warriors demonize salt and fat. But we need a daily salt intake to counter salt-loss through perspiration and the research shows that people on salt-restricted diets die SOONER. And Eskimos eat huge amounts of fat with no apparent ill-effects. And the average home-cooked roast dinner has LOTS of fat. Will we ban roast dinners?
6). The foods restricted are often no more calorific than those permitted -- such as milk and fruit-juice drinks.
7). Tendency to weight is mostly genetic and is therefore not readily susceptible to voluntary behaviour change.
8). And when are we going to ban cheese? Cheese is a concentrated calorie bomb and has lots of that wicked animal fat in it too. Wouldn't we all be better off without it? And what about butter and margarine? They are just about pure fat. Surely they should be treated as contraband in kids' lunchboxes! [/sarcasm].
9). And how odd it is that we never hear of the huge American study which showed that women who eat lots of veggies have an INCREASED risk of stomach cancer? So the official recommendation to eat five lots of veggies every day might just be creating lots of cancer for the future! It's as plausible (i.e. not very) as all the other dietary "wisdom" we read about fat etc.
10). And will "this generation of Western children be the first in history to lead shorter lives than their parents did"? This is another anti-fat scare that emanates from a much-cited editorial in a prominent medical journal that said so. Yet this editorial offered no statistical basis for its opinion -- an opinion that flies directly in the face of the available evidence.
Even statistical correlations far stronger than anything found in medical research may disappear if more data is used. A remarkable example from Sociology:"The modern literature on hate crimes began with a remarkable 1933 book by Arthur Raper titled The Tragedy of Lynching. Raper assembled data on the number of lynchings each year in the South and on the price of an acre's yield of cotton. He calculated the correlation coefficient between the two series at -0.532. In other words, when the economy was doing well, the number of lynchings was lower.... In 2001, Donald Green, Laurence McFalls, and Jennifer Smith published a paper that demolished the alleged connection between economic conditions and lynchings in Raper's data. Raper had the misfortune of stopping his analysis in 1929. After the Great Depression hit, the price of cotton plummeted and economic conditions deteriorated, yet lynchings continued to fall. The correlation disappeared altogether when more years of data were added."So we must be sure to base our conclusions on ALL the data. But in medical research, data selectivity and the "overlooking" of discordant research findings is epidemic.
"What we should be doing is monitoring children from birth so we can detect any deviations from the norm at an early stage and action can be taken". Who said that? Joe Stalin? Adolf Hitler? Orwell's "Big Brother"? The Spanish Inquisition? Generalissimo Francisco Franco Bahamonde? None of those. It was Dr Colin Waine, chairman of Britain's National Obesity Forum. What a fine fellow!
*********************
12 March, 2008
Diesel fumes trigger speculation
Hey! Who knew? People don't like breathing in diesel fumes!
INHALING diesel exhaust triggers a stress response in the brain that may have damaging long-term effects on brain function, Dutch researchers said. Previous studies have found very small particles of soot, or nanoparticles, are able to travel from the nose and lodge in the brain. But this is the first time researchers have demonstrated a change in brain activity. "We can only speculate what these effects may mean for the chronic exposure to air pollution encountered in busy cities where the levels of such soot particles can be very high," said lead researcher Paul Borm from Zuyd University. "It is conceivable that the long-term effects of exposure to traffic nanoparticles may interfere with normal brain function and information processing."
Prof Borm and his team put 10 volunteers in a room filled with exhaust from a diesel engine for one hour and monitored their brain waves with an electroencephalograph (EEG). The level of fumes was similar to that found on a busy road or in a garage. After about 30 minutes, brain wave patterns displayed a stress response, suggesting changes in information processing in the brain cortex.
Further research is needed to determine the clinical effect of this stress and whether it has any long-term impact on verbal and non-verbal intelligence or memory abilities. Still, the result appears to be another black mark for nanoparticles found in traffic fumes, which have already been linked with increased rates of respiratory and cardiovascular disease. The study was published in the journal Particle and Fibre Toxicology and is available online at http://www.particleandfibretoxicology.com/.
Source
The honey cure
At 42 British pounds for a 120g jar, the world’s most expensive honey recently went on sale in Harrods. Life Mel has a list of purported health benefits as long as your arm ? the scientists who created it claim the usual nutritional advantages associated with honey are maximised because the bees that produce it gather pollen from herbs such as Siberian ginseng, echinacea and Uncaria tomentosa that boost the immune system. They say that 2 tsp of Life Mel honey a day, on an empty stomach, sucked slowly, will supply a shot of antioxidants that leave you better able to fight illness and disease.
Life Mel has already established a reputation as something of a miracle nectar: a study published in the respected Medical Oncology journal last year showed that 12 out of 30 cancer patients given the honey after chemotherapy did not experience the usual plummeting white blood-cell count; other patients reported improvements in their quality of life. However, even the researchers, at Sieff hospital in Israel, where the honey is produced, and Oldchurch Hospital in Romford, Essex, admit the sample was small, and that the proven benefits are slight.
But haven’t we heard it all before? Is honey really a cureall, or is this just a load of hype? Trials conducted at the honey research centre at Waikato University, New Zealand, look more promising. The director of the centre, Professor Peter Molan, has focused his investigations on another super-honey, manuka, which is produced by bees that collect pollen from the manuka bush, which grows wild in New Zealand.
According to Molan, all types of honey contain hydrogen peroxide -- once used in hospitals as a disinfectant for wounds because of its antibacterial properties -- which is produced from an enzyme, glucose oxidase, which the bees add to nectar. Manuka honey appears to contain other beneficial ingredients, yet to be identified, which help it to fight bacteria. Molan has found that eating 3 tsp manuka honey a day can help fight throat infections and reduce gum disease, as well as maintain good digestive health. He has also shown that, when eaten regularly, manuka also aids memory and reduces feelings of anxiety.
At Aintree Hospital in Liverpool and at the University of Wales, manuka honey has been shown to combat MRSA when applied to wounds; other researchers have suggested it may also be useful as a dressing for eczema, sunburn and acne.
Despite these benefits, experts are not convinced that we should all be dipping a spoon into the jar every day. Lisa Miles, a nutrition scientist with the British Nutrition Foundation, points out that while honey may have its uses in specific medical settings, it contains 16 more calories (64) per tbsp than sugar (48). “It is just liquid sugar,” she says. “It has a reputation as being healthier than sugar, but, nutritionally, there are few advantages. Honey is 75% sugar and counts as added sugar in the diet, so don’t be fooled.” The only thing guaranteed to happen when you eat more of it, she says, is that you will put on weight.
Source
****************
Just some problems with the "Obesity" war:
1). It tries to impose behavior change on everybody -- when most of those targeted are not obese and hence have no reason to change their behaviour. It is a form of punishing the innocent and the guilty alike. (It is also typical of Leftist thinking: Scorning the individual and capable of dealing with large groups only).
2). The longevity research all leads to the conclusion that it is people of MIDDLING weight who live longest -- not slim people. So the "epidemic" of obesity is in fact largely an "epidemic" of living longer.
3). It is total calorie intake that makes you fat -- not where you get your calories. Policies that attack only the source of the calories (e.g. "junk food") without addressing total calorie intake are hence pissing into the wind. People involuntarily deprived of their preferred calorie intake from one source are highly likely to seek and find their calories elsewhere.
4). So-called junk food is perfectly nutritious. A big Mac meal comprises meat, bread, salad and potatoes -- which is a mainstream Western diet. If that is bad then we are all in big trouble.
5). Food warriors demonize salt and fat. But we need a daily salt intake to counter salt-loss through perspiration and the research shows that people on salt-restricted diets die SOONER. And Eskimos eat huge amounts of fat with no apparent ill-effects. And the average home-cooked roast dinner has LOTS of fat. Will we ban roast dinners?
6). The foods restricted are often no more calorific than those permitted -- such as milk and fruit-juice drinks.
7). Tendency to weight is mostly genetic and is therefore not readily susceptible to voluntary behaviour change.
8). And when are we going to ban cheese? Cheese is a concentrated calorie bomb and has lots of that wicked animal fat in it too. Wouldn't we all be better off without it? And what about butter and margarine? They are just about pure fat. Surely they should be treated as contraband in kids' lunchboxes! [/sarcasm].
9). And how odd it is that we never hear of the huge American study which showed that women who eat lots of veggies have an INCREASED risk of stomach cancer? So the official recommendation to eat five lots of veggies every day might just be creating lots of cancer for the future! It's as plausible (i.e. not very) as all the other dietary "wisdom" we read about fat etc.
10). And will "this generation of Western children be the first in history to lead shorter lives than their parents did"? This is another anti-fat scare that emanates from a much-cited editorial in a prominent medical journal that said so. Yet this editorial offered no statistical basis for its opinion -- an opinion that flies directly in the face of the available evidence.
Even statistical correlations far stronger than anything found in medical research may disappear if more data is used. A remarkable example from Sociology:"The modern literature on hate crimes began with a remarkable 1933 book by Arthur Raper titled The Tragedy of Lynching. Raper assembled data on the number of lynchings each year in the South and on the price of an acre's yield of cotton. He calculated the correlation coefficient between the two series at -0.532. In other words, when the economy was doing well, the number of lynchings was lower.... In 2001, Donald Green, Laurence McFalls, and Jennifer Smith published a paper that demolished the alleged connection between economic conditions and lynchings in Raper's data. Raper had the misfortune of stopping his analysis in 1929. After the Great Depression hit, the price of cotton plummeted and economic conditions deteriorated, yet lynchings continued to fall. The correlation disappeared altogether when more years of data were added."So we must be sure to base our conclusions on ALL the data. But in medical research, data selectivity and the "overlooking" of discordant research findings is epidemic.
"What we should be doing is monitoring children from birth so we can detect any deviations from the norm at an early stage and action can be taken". Who said that? Joe Stalin? Adolf Hitler? Orwell's "Big Brother"? The Spanish Inquisition? Generalissimo Francisco Franco Bahamonde? None of those. It was Dr Colin Waine, chairman of Britain's National Obesity Forum. What a fine fellow!
*********************
11 March, 2008
Amusing: Another one of the hoary attacks on white bread
Such attacks go back to the 1920s at least. The study is a classical example of GIGO (garbage in, garbage out). Summarizing a lot of studies that are themselves just epidemiological speculation tells us nothing
Eating white bread and sugary breakfast cereals can increase the risk of diabetes, heart disease and even cancer, new Australian research suggests. A world-first study by Sydney scientists has found conclusive evidence that a high GI diet, generally rich in food that is burnt by the body quickly, leads to a higher risk of common lifestyle diseases.
The Glycemic Index (GI) is a measure of how different foods affect your blood glucose levels, with those that are "low GI" released more slowly and deemed better for health. A team of nutrition experts at the University of Sydney evaluated 37 diet studies involving nearly two million people worldwide to analyse the effect of eating high GI foods, which are usually highly processed. The study, published in the American Journal of Clinical Nutrition, found a link between a high GI diet and a high risk of type 2 diabetes and heart disease. The diet was also linked to gall stones and some types of cancer.
"The key message from this study," says lead author Alan Barclay, "is that the GI of your diet is a powerful predictor of disease risk. "Grandma was right, you are what you eat." He said the link with diabetes was "not surprising" because eating high GI foods inflates your blood glucose and insulin levels. "You may literally 'wear out' your pancreas over time [Crap! In the human body, a much-used function tends to get stronger] and eventually it may lead to type 2 diabetes in older age," Mr Barclay said.
The researchers were more surprised by the "strong relationship" between GI and cancer. High GI foods cause constant spikes in blood glucose which increase insulin and a related substance called 'insulin-like growth factor one', both of which have been shown to increase the risk of developing cancer. "Other research shows that a high GI diet tends to reduce 'good' HDL cholesterol levels and raise triglycerides levels; bad news for cardiovascular diseases," he said. "And people with low HDL cholesterol and high triglyceride levels are more prone to gall stones."
The researchers said their findings support eating a low GI diet to maintain healthy weight and help avoid disease. Caryl Nowson, a professor of nutrition and ageing at Deakin University in Melbourne, said because high GI foods were typically high in fat and sugar and low in fibre, they were also ready known to be linked with disease. "This review is just a new way of breaking down dietary information we already have," Prof Nowson said. She said while the benefits of eating according to GI rating had been proven, it was just one of many ways to structure a healthy diet. "If you focus on having a classically balanced diet high in fibre and low in sugar, fat and refined foods you'll find you're eating relatively low GI anyway," Prof Nowson said.
Source
No sex for fatties?
This stuff is as yet unpublished but it sounds like the usual epidemiological crap -- based on self-reports, no doubt
Fat men who care more about sex than losing weight should realise there is a good possibility they will have erectile dysfunction, an obesity expert says. The head of Adelaide University’s medical school, Professor Gary Wittert, said men should take note of research linking obesity to erectile dysfunction. “Australian men care about erection problems, perhaps more so than possible cardiovascular disease,” Prof Wittert said. “This may present an opportunity to improve communication about the benefits of weight loss.”
Prof Wittert said that while many men were aware of several health problems which were caused by obesity, difficulties getting an erection were less known. “It’s becoming well known that there are high levels of obesity in Australian men and that this has significant consequences for chronic diseases, both physical and psychological,” he said. “What is less well known is that not only blood vessels to the heart are affected by obesity but similar effects occur with the blood vessels to the penis with resulting erectile dysfunction and poor urinary tract function.”
Prof Wittert will release some of the findings of a major study into the health and ageing of Australian men tomorrow afternoon. As part of the Florey Adelaide Male Ageing Study, about 1,000 men were examined in an attempt to identify the key factors that determined their reproductive, physical and emotional health.
Source
****************
Just some problems with the "Obesity" war:
1). It tries to impose behavior change on everybody -- when most of those targeted are not obese and hence have no reason to change their behaviour. It is a form of punishing the innocent and the guilty alike. (It is also typical of Leftist thinking: Scorning the individual and capable of dealing with large groups only).
2). The longevity research all leads to the conclusion that it is people of MIDDLING weight who live longest -- not slim people. So the "epidemic" of obesity is in fact largely an "epidemic" of living longer.
3). It is total calorie intake that makes you fat -- not where you get your calories. Policies that attack only the source of the calories (e.g. "junk food") without addressing total calorie intake are hence pissing into the wind. People involuntarily deprived of their preferred calorie intake from one source are highly likely to seek and find their calories elsewhere.
4). So-called junk food is perfectly nutritious. A big Mac meal comprises meat, bread, salad and potatoes -- which is a mainstream Western diet. If that is bad then we are all in big trouble.
5). Food warriors demonize salt and fat. But we need a daily salt intake to counter salt-loss through perspiration and the research shows that people on salt-restricted diets die SOONER. And Eskimos eat huge amounts of fat with no apparent ill-effects. And the average home-cooked roast dinner has LOTS of fat. Will we ban roast dinners?
6). The foods restricted are often no more calorific than those permitted -- such as milk and fruit-juice drinks.
7). Tendency to weight is mostly genetic and is therefore not readily susceptible to voluntary behaviour change.
8). And when are we going to ban cheese? Cheese is a concentrated calorie bomb and has lots of that wicked animal fat in it too. Wouldn't we all be better off without it? And what about butter and margarine? They are just about pure fat. Surely they should be treated as contraband in kids' lunchboxes! [/sarcasm].
9). And how odd it is that we never hear of the huge American study which showed that women who eat lots of veggies have an INCREASED risk of stomach cancer? So the official recommendation to eat five lots of veggies every day might just be creating lots of cancer for the future! It's as plausible (i.e. not very) as all the other dietary "wisdom" we read about fat etc.
10). And will "this generation of Western children be the first in history to lead shorter lives than their parents did"? This is another anti-fat scare that emanates from a much-cited editorial in a prominent medical journal that said so. Yet this editorial offered no statistical basis for its opinion -- an opinion that flies directly in the face of the available evidence.
Even statistical correlations far stronger than anything found in medical research may disappear if more data is used. A remarkable example from Sociology:"The modern literature on hate crimes began with a remarkable 1933 book by Arthur Raper titled The Tragedy of Lynching. Raper assembled data on the number of lynchings each year in the South and on the price of an acre's yield of cotton. He calculated the correlation coefficient between the two series at -0.532. In other words, when the economy was doing well, the number of lynchings was lower.... In 2001, Donald Green, Laurence McFalls, and Jennifer Smith published a paper that demolished the alleged connection between economic conditions and lynchings in Raper's data. Raper had the misfortune of stopping his analysis in 1929. After the Great Depression hit, the price of cotton plummeted and economic conditions deteriorated, yet lynchings continued to fall. The correlation disappeared altogether when more years of data were added."So we must be sure to base our conclusions on ALL the data. But in medical research, data selectivity and the "overlooking" of discordant research findings is epidemic.
"What we should be doing is monitoring children from birth so we can detect any deviations from the norm at an early stage and action can be taken". Who said that? Joe Stalin? Adolf Hitler? Orwell's "Big Brother"? The Spanish Inquisition? Generalissimo Francisco Franco Bahamonde? None of those. It was Dr Colin Waine, chairman of Britain's National Obesity Forum. What a fine fellow!
*********************
10 March, 2008
Replacing the Fatropolis with Fit Towns
New `healthy towns' that encourage people to walk more, eat the right kind of food and stay forever fit take repression to a new level. Comment from Britain
`Salt `could fuel childhood obesity"' whispered one headline this week; `World is in obesity crisis' roared another. It seems barely a day passes without some report or policy announcement reminding us that the deep-fried fruits of modernity are dragging us to our gluttonous, sedentry doom. Change your ways, they exhort. However, if recent plans to redesign our towns as `fit towns' are anything to go by, instruction and guilt-tripping are giving way to something far more repressive.
The possibility of replanning and redesigning our towns in order to encourage healthy lifestyles was originally raised last November by UK health secretary, Alan Johnson. Citing `international evidence and research' that shows we `need a large-scale approach across the whole community to help tackle obesity' he suggested proposed eco-towns should also be made `healthy towns. through their layout, facilities and construction'. He concluded that our `built environment [must] do more to help people make physical activity a normal part of everyday life' (1).
In Boston last Sunday, the conference of the American Association for the Advancement of Science saw a similarly depressing nod to lifestyle management. Professor Philip James of the London School of Hygiene and Tropical Medicine and, more importantly, chairman of the Brave-New-World-sounding International Obesity Taskforce, declared: `The environment in which we live is the overwhelming factor amplifying the obesity epidemic'. He continued, arguing that it was na‹ve to place `the onus on individuals making "healthier choices" while the environment in which we live is the overwhelming factor amplifying the epidemic' (2). Rena Wing of Brown University echoed the pessimistic view of individuals' capacity to make what the holier-than-thou alliance of policy makers and experts deem the right choices: `We live in an obesogenic environment that relies heavily on fast food, automobiles and remote controls - all of which can be labelled as "toxic" to maintaining a healthy weight.' (3)
The overarching aim of remaking our fatropolises as fit-towns is all too clear: as we can't be trusted to make the correct decisions, we, the public, shall be forcibly diverted from the dual-carriage way of temptation on to the fully pedestrianised area of righteousness.
Admittedly, some of the measures suggested seem innocuous enough. Stairwells, for instance, should be made to look less like badly lit fire escapes and made a bit more glamorous, spiral perhaps. And parks should be better maintained, with better lighting. Other proposals, however, are all too restrictive. For instance, some of the proposed towns should give priority to pedestrians and cyclists over the car, perhaps providing office premises with bike-only parking. And the bane of the obesity warrior's crusade, the fast food outlet, must never be erected near parks or schools. (4)
Of course there is nothing especially novel about urban planning, nor its political underpinnings. Take Baron Haussmann's reconstruction of Paris between 1852 and 1870. With memories of the revolutionary commune of 1848 still fresh, Haussmann, under Napoleon III's instructions, demolished vast swathes of the city and built long, sweeping boulevards in their place. In doing so he both inhibited the erection of barricades and made it easy for the army to gain access. In other words the attempt to maintain social order was embodied in Parisians' lived environment.
Indeed, on a more general scale, our environment has long reflected the ruling needs of the moment. Richard Sennet in his 1997 book, The Fall of Public Man, saw in the bustling thoroughfares and concourses of the modern city the predominance of the private individual of bourgeois myth. Public space was made a mere function of private motion, of getting from a to b as quickly as possible. Strolling, meandering, and leisurely interacting with our fellows were incompatible with the manic industriousness demanded of the bourgeois individual.
Accepting that urban planning - the regulation of public space - or indeed, its absence, has always provided a mirror of society, then what does the notion of the fit town reflect? Whilst it is not concerned, as Napoleon III was, with the threat posed by social disorder, it is still dealing with a threat. This time however, the threat is not embodied in, say, the communards - it is not external at all. It is, rather, internal to each and every one of us. Fit towns combat our tendency to consume and to seek convenience - we are our own worst enemies. While fast food, remote controls or electric tooth brushes save labour, they're killing us.
Fit towns embody more than the war on obesity. They wage war on our consuming passions per se, be it a desire to light-up, to booze, or to go large on a Big Mac and fries. Above all they fight our tendency to err.
To borrow, then, from the increasingly martial lexicon of government policy, fit towns are located on the frontier of the war on error. The result, from the jarring positivity of phrases like the International Obesity Taskforce, or, indeed, the `fit town' itself is an environment every bit as deeply repressive as that evoked in their different ways by George Orwell or Aldous Huxley.
Source
Heart disease: we need medicine not moralism
Fear of rising heart deaths is unfounded. And if we're serious about lowering the death rate even further, we need better treatment not lifestyle lectures
This week, a number of news headlines have highlighted the deadly threat of heart disease in Britain: `Bank crises "increase rate of heart attacks"`, warned the UK Guardian on Tuesday. The day before, The Times (London) cautioned that `Young adults' inactivity puts them at risk of heart attack'.
The Guardian report is based on research from the University of Cambridge. Data from the World Bank and World Health Organisation over a 40-year period was analysed at Cambridge, where the researchers concluded that between 1,280 and 5,130 Brits `could die from heart attacks if there was a widespread repeat of the Northern Rock banking crisis' (1). Lead researcher David Stuckler said: `To put this effect in perspective, this is more than 10 times the number of British troops who have died in Iraq.' The researchers found that `cardiac deaths surge briefly and regularly every time there is a systemic bank failure' and it is the elderly that are at greatest risk.
But those of us aged 35 to 54 had better not be too complacent, we're told, because our lives may be cut short by our `live-now' lifestyles. Simon Capewell, professor of clinical epidemiology at the University of Liverpool, said: `The flattening trends in mortality rates among young adults suggest that the cardiovascular disease epidemic is not being controlled.' He warned: `The party is over and complacency runs a high risk.'
Having recently lost both my mother and my uncle to heart disease, I am not about to advocate complacency. It is estimated that in the European Union, cardiovascular disease kills over two million people every year. Still, a little perspective would not go amiss. The fact is that despite the impression given by various newspaper headlines, heart disease is not on the rise. Instead, the concern voiced by some experts, and blown out of all proportion by others, is that the dramatic decrease in deaths from heart disease over the last few decades has started to flatten out.
In my view, the experts should be concerned. They should be continually trying to reduce deaths from heart disease. Clearly, a hell of lot more can be done to improve medical intervention: my mother died from a massive heart attack several months after being put on a waiting list for heart surgery. If she had been given the treatment she needed earlier she may still have been alive today. If the medical establishment could spend a little more time putting its own house in order and a little less time lecturing us about our `live-now' lifestyles, we may all be better off.
The warning that up to 5,000 people could lose their lives if we faced a massive banking crisis may be shocking. But these figures were arrived at using not-entirely-reliable computer models comparing associations between banking crises and cardiovascular disease deaths. Also, when we consider the Cambridge study's figures alongside the fact that there were 68,230 fewer deaths from heart disease in 2000 than there were in 1981 in England and Wales, the potential effect of a financial crisis no longer seems so shocking.
There was a 62 per cent reduction in deaths from heart disease among men and a 45 per cent reduction among women over two decades from 1981. Various factors have contributed to this dramatic decrease. A large-scale study in 2004 by Capewell indicates that 58 per cent of this decrease is due to a reduction in certain risk factors, such as smoking, and 42 per cent is due to the availability of more advanced medical and surgical treatments - although this study, too, was the product of a computer model (2). Today's heart scare is the result of scaremongers twisting what is actually a good news story: the dramatic decline in deaths from heart disease over the past 20 years. That this decline seems to be levelling off should be investigated, of course, but it should also be seen in the context of an overall successful war against death from heart disease.
We all know smoking is bad for us and don't need to be lectured any more about that. The effect of obesity and diet on our health and our hearts is much more uncertain and, to the extent that there is a problem, there is as yet no simple solution like there is with smoking - we can't exactly quit food. So, rather than telling us how to live, physicians should now concentrate on reducing mortality rates further by improving the availability and efficacy of medical intervention.
Source
****************
Just some problems with the "Obesity" war:
1). It tries to impose behavior change on everybody -- when most of those targeted are not obese and hence have no reason to change their behaviour. It is a form of punishing the innocent and the guilty alike. (It is also typical of Leftist thinking: Scorning the individual and capable of dealing with large groups only).
2). The longevity research all leads to the conclusion that it is people of MIDDLING weight who live longest -- not slim people. So the "epidemic" of obesity is in fact largely an "epidemic" of living longer.
3). It is total calorie intake that makes you fat -- not where you get your calories. Policies that attack only the source of the calories (e.g. "junk food") without addressing total calorie intake are hence pissing into the wind. People involuntarily deprived of their preferred calorie intake from one source are highly likely to seek and find their calories elsewhere.
4). So-called junk food is perfectly nutritious. A big Mac meal comprises meat, bread, salad and potatoes -- which is a mainstream Western diet. If that is bad then we are all in big trouble.
5). Food warriors demonize salt and fat. But we need a daily salt intake to counter salt-loss through perspiration and the research shows that people on salt-restricted diets die SOONER. And Eskimos eat huge amounts of fat with no apparent ill-effects. And the average home-cooked roast dinner has LOTS of fat. Will we ban roast dinners?
6). The foods restricted are often no more calorific than those permitted -- such as milk and fruit-juice drinks.
7). Tendency to weight is mostly genetic and is therefore not readily susceptible to voluntary behaviour change.
8). And when are we going to ban cheese? Cheese is a concentrated calorie bomb and has lots of that wicked animal fat in it too. Wouldn't we all be better off without it? And what about butter and margarine? They are just about pure fat. Surely they should be treated as contraband in kids' lunchboxes! [/sarcasm].
9). And how odd it is that we never hear of the huge American study which showed that women who eat lots of veggies have an INCREASED risk of stomach cancer? So the official recommendation to eat five lots of veggies every day might just be creating lots of cancer for the future! It's as plausible (i.e. not very) as all the other dietary "wisdom" we read about fat etc.
10). And will "this generation of Western children be the first in history to lead shorter lives than their parents did"? This is another anti-fat scare that emanates from a much-cited editorial in a prominent medical journal that said so. Yet this editorial offered no statistical basis for its opinion -- an opinion that flies directly in the face of the available evidence.
Even statistical correlations far stronger than anything found in medical research may disappear if more data is used. A remarkable example from Sociology:"The modern literature on hate crimes began with a remarkable 1933 book by Arthur Raper titled The Tragedy of Lynching. Raper assembled data on the number of lynchings each year in the South and on the price of an acre's yield of cotton. He calculated the correlation coefficient between the two series at -0.532. In other words, when the economy was doing well, the number of lynchings was lower.... In 2001, Donald Green, Laurence McFalls, and Jennifer Smith published a paper that demolished the alleged connection between economic conditions and lynchings in Raper's data. Raper had the misfortune of stopping his analysis in 1929. After the Great Depression hit, the price of cotton plummeted and economic conditions deteriorated, yet lynchings continued to fall. The correlation disappeared altogether when more years of data were added."So we must be sure to base our conclusions on ALL the data. But in medical research, data selectivity and the "overlooking" of discordant research findings is epidemic.
"What we should be doing is monitoring children from birth so we can detect any deviations from the norm at an early stage and action can be taken". Who said that? Joe Stalin? Adolf Hitler? Orwell's "Big Brother"? The Spanish Inquisition? Generalissimo Francisco Franco Bahamonde? None of those. It was Dr Colin Waine, chairman of Britain's National Obesity Forum. What a fine fellow!
*********************
9 March, 2008
Taking to drink could cut heart disease risk (Maybe)
A new offering to the cholesterol religion
Middle-aged people who have never drunk alcohol can cut their risk of heart disease sharply by taking to the bottle - especially if it contains wine. US doctors have found that the new drinkers rarely overdid it, stuck to safe limits and cut their risk of heart disease by 38 per cent in four years.
Although drinking moderately has been shown to have benefits in many studies, doctors have until now always been unwilling to recommend non-drinkers to take it up. The new results may embolden them. A team from the Medical University of South Carolina looked at heart disease in 7,697 men and women aged 45 to 64, all of whom started out as non-drinkers. Of these, 6 per cent became moderate drinkers during the ten-year study. Typically this amounted to two drinks a day for men and one for women.
After an average of four years the new drinkers were found to have a 38 per cent lower chance of developing heart or artery disease than those who continued to spurn alcohol. New drinkers who consumed only wine appeared to benefit most, according to the findings published in The American Journal of Medicine. Their risk of a cardiovascular event such as a heart attack or stroke was 68 per cent lower than non-drinkers. People who preferred other drinks, such as beer or spirits, had an advantage over teetotallers, but not to a significant degree. There was no overall effect on death rates, probably because the study was too short to detect any decline through heart disease, or any increase because of cancer.
Dana King, who led the team, wrote in the paper: "A substantial cardiovascular benefit from adopting moderate alcohol drinking in middle age appears supported by the study. "The findings suggest that, for carefully selected individuals, a `heart-healthy diet' may include limited alcohol consumption even among individuals who have not included alcohol previously."
Researchers saw differences in cholesterol level and blood pressure between the drinkers and non-drinkers. Levels of "bad" low-density lipoprotein cholesterol were significantly lower among new drinkers, and levels of "good" high-density lipoprotein cholesterol higher.
Source
Aspirin could help to reduce risk of breast cancer by 20%
But aspirin routinely causes stomach bleeding! Surely we can't have that? Ban aspirin!
Drugs such as aspirin may help to reduce the risk of breast cancer by about 20 per cent, according to a review of past studies. Experts analysed 21 studies involving more than 37,000 women and found an overall decreased risk for those taking non-steroidal anti-inflammatory drugs (NSAIDs). They could also play a role in treating women who have breast cancer.
The researchers said that more studies were needed on the ideal type of drug, dose and duration, and that they had not considered the side-effects. High doses can increase the risk of heart attacks and other health problems. The researchers concluded: "There may be a role for NSAIDs in combination with endocrine therapies as either an adjuvant or palliative treatment for women with established breast cancer."
Ian Fentiman, Professor of Oncology at Guy's and St Thomas' NHS Foundation Trust, carried out the study, published in the International Journal of Clinical Practice.
Source
****************
Just some problems with the "Obesity" war:
1). It tries to impose behavior change on everybody -- when most of those targeted are not obese and hence have no reason to change their behaviour. It is a form of punishing the innocent and the guilty alike. (It is also typical of Leftist thinking: Scorning the individual and capable of dealing with large groups only).
2). The longevity research all leads to the conclusion that it is people of MIDDLING weight who live longest -- not slim people. So the "epidemic" of obesity is in fact largely an "epidemic" of living longer.
3). It is total calorie intake that makes you fat -- not where you get your calories. Policies that attack only the source of the calories (e.g. "junk food") without addressing total calorie intake are hence pissing into the wind. People involuntarily deprived of their preferred calorie intake from one source are highly likely to seek and find their calories elsewhere.
4). So-called junk food is perfectly nutritious. A big Mac meal comprises meat, bread, salad and potatoes -- which is a mainstream Western diet. If that is bad then we are all in big trouble.
5). Food warriors demonize salt and fat. But we need a daily salt intake to counter salt-loss through perspiration and the research shows that people on salt-restricted diets die SOONER. And Eskimos eat huge amounts of fat with no apparent ill-effects. And the average home-cooked roast dinner has LOTS of fat. Will we ban roast dinners?
6). The foods restricted are often no more calorific than those permitted -- such as milk and fruit-juice drinks.
7). Tendency to weight is mostly genetic and is therefore not readily susceptible to voluntary behaviour change.
8). And when are we going to ban cheese? Cheese is a concentrated calorie bomb and has lots of that wicked animal fat in it too. Wouldn't we all be better off without it? And what about butter and margarine? They are just about pure fat. Surely they should be treated as contraband in kids' lunchboxes! [/sarcasm].
9). And how odd it is that we never hear of the huge American study which showed that women who eat lots of veggies have an INCREASED risk of stomach cancer? So the official recommendation to eat five lots of veggies every day might just be creating lots of cancer for the future! It's as plausible (i.e. not very) as all the other dietary "wisdom" we read about fat etc.
10). And will "this generation of Western children be the first in history to lead shorter lives than their parents did"? This is another anti-fat scare that emanates from a much-cited editorial in a prominent medical journal that said so. Yet this editorial offered no statistical basis for its opinion -- an opinion that flies directly in the face of the available evidence.
Even statistical correlations far stronger than anything found in medical research may disappear if more data is used. A remarkable example from Sociology:"The modern literature on hate crimes began with a remarkable 1933 book by Arthur Raper titled The Tragedy of Lynching. Raper assembled data on the number of lynchings each year in the South and on the price of an acre's yield of cotton. He calculated the correlation coefficient between the two series at -0.532. In other words, when the economy was doing well, the number of lynchings was lower.... In 2001, Donald Green, Laurence McFalls, and Jennifer Smith published a paper that demolished the alleged connection between economic conditions and lynchings in Raper's data. Raper had the misfortune of stopping his analysis in 1929. After the Great Depression hit, the price of cotton plummeted and economic conditions deteriorated, yet lynchings continued to fall. The correlation disappeared altogether when more years of data were added."So we must be sure to base our conclusions on ALL the data. But in medical research, data selectivity and the "overlooking" of discordant research findings is epidemic.
"What we should be doing is monitoring children from birth so we can detect any deviations from the norm at an early stage and action can be taken". Who said that? Joe Stalin? Adolf Hitler? Orwell's "Big Brother"? The Spanish Inquisition? Generalissimo Francisco Franco Bahamonde? None of those. It was Dr Colin Waine, chairman of Britain's National Obesity Forum. What a fine fellow!
*********************
8 March, 2008
Short people could live longer
And pigs might fly. Tall people are always shown as healthier in research
Evidence of a link between height and longevity has been found by scientists, suggesting that some short people will live longer than their taller peers. Normal variation in human height is due to a blend of environmental factors, notably diet, and genetic factors. Now one such inherited factor that could extend the human lifespan by as much as one third in theory has been uncovered, though it may come at the cost of a few inches in height.
The work also suggests that the [inappropriate] use of growth hormone as an anti-ageing medicine may actually be shortening lifespan. And it confirms the emerging view among scientists that rather than being a passive, haphazard process of wear and tear, some people may be blessed with genes that make them more likely to live to a ripe old age. [So that is new??]
Earlier work by a French team showed that mice lacking one copy of the gene IGF-1 live on average 26 per cent longer than normal, with females enjoying a bigger advantage (33 per cent increase in lifespan) than males (16 per cent increase). Damping down the same pathway of the metabolism also resulted in extension of lifespan in yeasts, worms, and flies too. And the same pathway is affected by diets low in calories, the only proven way to extend lifespan.
Now a study by Prof Nir Barzilai, Director, Institute for Aging Research, Albert Einstein College of Medicine, New York, reveals that the same gene is involved in the "oldest old" of people, revealing in the long run how to postpone the physiological ageing process.
Insulin-like growth factor (IGF-1) levels have previously been linked with both ageing and body size, with evidence showing that decreased levels of IGF-1 predispose the animals for short stature, but increased longevity. To determine if IGF-1 plays a role in human longevity, Prof Barzilai, Dr Yousin Suh and colleagues looked for variations in the gene within a group of Ashkenazi Jewish centenarians and their children.
The researchers used Ashkenazi individuals with no history of familial longevity, matched for age and sex as controls. Comparing the two groups, the researchers report in the Proceedings of the National Academy of Sciences that centenarians and their offspring were more likely to have a variety of mutations in the IGF-1 receptor which reduced the effects of the factor. As had been shown by the mouse work, the less active IGF-1 pathway had bigger effects on women than men and led to shorter stature.
The work shows that this pathway plays a role in human longevity, which provides new clues as to how to boost lifespan by damping down the action of IGF-1, and other molecules that play a part in this piece of metabolic machinery. "Practically, this discovery supports the notion that growth hormone, which is injected as anti-ageing medicine in the US (and other countries) maybe dangerous, because it is the people who have low growth hormone levels that are living longer," Prof Barzilai tells The Daily Telegraph. "So avoiding growth hormone may increase ones longevity."
The team does not yet know if longevity is assured by having low growth hormone action throughout life, or whether it is enough to have it decreased at a certain age. "The fact is that growth hormone levels and actions are decreased in old age," he adds.
His team has found other longevity genes - notably CETP and APOC3 - that are also under study to see if there is potential to make anti ageing drugs, though it is too early to speculate on when people will benefit from this understanding.
Source
New 'thin pill' could replace surgery
A new generation of diet pills that could achieve the same dramatic weight loss as surgery could be available within a decade. A team at University College London is working towards developing a weight loss pill that makes people feel they are full after eating a small amount of food. The stomach has to expand to digest food, the basic process by which the body harvests calories from meals, but scientists have found a way of stopping this from happening.
The pill could offer an alternative to stomach stapling - gastroplasty - in which a band or surgery is used to reduce the size of the stomach. This can result in weight loss of up to 7st in a year. However, surgery can be risky with one in every 100 patients dying within 12 months. The potential new drug is described in the Journal of Pharmacology and Experimental Therapeutics by Dr Brian King and Dr Andrea Townsend-Nicholson. "It is chemical gastric banding," said Dr Townsend-Nicholson, adding that the pill could be available for use within five to 10 years.
The team found two proteins - P2Y1 and P2Y11 - which are receptors that pick up signals from nerves to control the size of the gut. These were identified in the guinea pig, but are also present in humans. Dr King said: "This would be a brand new approach to weight control." Dr Brian King says: "The mechanisms we have identified are important to the normal workings of the stomach - a hollow organ which actively relaxes to help accommodate the size of your meal.
The human stomach has a 'resting' internal volume of 75 millilitres (one tenth of a pint) but, by relaxing its muscular wall, can expand to an internal volume of two litres (3.5 pints) or more - a 25-fold increase in the volume it can accept. "This expansion is controlled by nerves inside the stomach wall and these release molecules that stimulate the P2Y1 and P2Y11 receptor proteins embedded in muscle cells in the gut wall. The mechanism of this slow relaxation of the stomach might represent a future drug target in the fight to control weight gain and reverse obesity. "We are looking to identify drugs that would block the P2Y11 receptor and, therefore, prevent slow relaxation of the stomach. As a result of blocking the P2Y11-based mechanism, meal size would be smaller, offering the person a better chance of regulating their food intake.
"This would be a brand new approach to weight control. At present, the most successful way to help obese patients lose weight is gastric banding or stomach stapling, both of which reduce the maximum volume of the stomach. "But these are also tricky surgical procedures, not without attendant risks. A pill that could replace this surgery, yet have the same effect, might be a useful alternative."
If the gastric bypass is anything to go by, there may be side effects. In the wake of stomach stapling, high fibre foods and foods with a more dense, natural consistency can become very difficult to eat relative to highly refined foods. There can be vomiting and severe discomfort if food is not properly chewed or if food is eaten too quickly. However, the UCL team believes that any possible side effects of chemical gastric banding are likely to outweigh the adverse health consequences of obesity.
Figures released in January showed that more than one million prescriptions for obesity drugs are now given to patients by GPs.
Source
****************
Just some problems with the "Obesity" war:
1). It tries to impose behavior change on everybody -- when most of those targeted are not obese and hence have no reason to change their behaviour. It is a form of punishing the innocent and the guilty alike. (It is also typical of Leftist thinking: Scorning the individual and capable of dealing with large groups only).
2). The longevity research all leads to the conclusion that it is people of MIDDLING weight who live longest -- not slim people. So the "epidemic" of obesity is in fact largely an "epidemic" of living longer.
3). It is total calorie intake that makes you fat -- not where you get your calories. Policies that attack only the source of the calories (e.g. "junk food") without addressing total calorie intake are hence pissing into the wind. People involuntarily deprived of their preferred calorie intake from one source are highly likely to seek and find their calories elsewhere.
4). So-called junk food is perfectly nutritious. A big Mac meal comprises meat, bread, salad and potatoes -- which is a mainstream Western diet. If that is bad then we are all in big trouble.
5). Food warriors demonize salt and fat. But we need a daily salt intake to counter salt-loss through perspiration and the research shows that people on salt-restricted diets die SOONER. And Eskimos eat huge amounts of fat with no apparent ill-effects. And the average home-cooked roast dinner has LOTS of fat. Will we ban roast dinners?
6). The foods restricted are often no more calorific than those permitted -- such as milk and fruit-juice drinks.
7). Tendency to weight is mostly genetic and is therefore not readily susceptible to voluntary behaviour change.
8). And when are we going to ban cheese? Cheese is a concentrated calorie bomb and has lots of that wicked animal fat in it too. Wouldn't we all be better off without it? And what about butter and margarine? They are just about pure fat. Surely they should be treated as contraband in kids' lunchboxes! [/sarcasm].
9). And how odd it is that we never hear of the huge American study which showed that women who eat lots of veggies have an INCREASED risk of stomach cancer? So the official recommendation to eat five lots of veggies every day might just be creating lots of cancer for the future! It's as plausible (i.e. not very) as all the other dietary "wisdom" we read about fat etc.
10). And will "this generation of Western children be the first in history to lead shorter lives than their parents did"? This is another anti-fat scare that emanates from a much-cited editorial in a prominent medical journal that said so. Yet this editorial offered no statistical basis for its opinion -- an opinion that flies directly in the face of the available evidence.
Even statistical correlations far stronger than anything found in medical research may disappear if more data is used. A remarkable example from Sociology:"The modern literature on hate crimes began with a remarkable 1933 book by Arthur Raper titled The Tragedy of Lynching. Raper assembled data on the number of lynchings each year in the South and on the price of an acre's yield of cotton. He calculated the correlation coefficient between the two series at -0.532. In other words, when the economy was doing well, the number of lynchings was lower.... In 2001, Donald Green, Laurence McFalls, and Jennifer Smith published a paper that demolished the alleged connection between economic conditions and lynchings in Raper's data. Raper had the misfortune of stopping his analysis in 1929. After the Great Depression hit, the price of cotton plummeted and economic conditions deteriorated, yet lynchings continued to fall. The correlation disappeared altogether when more years of data were added."So we must be sure to base our conclusions on ALL the data. But in medical research, data selectivity and the "overlooking" of discordant research findings is epidemic.
"What we should be doing is monitoring children from birth so we can detect any deviations from the norm at an early stage and action can be taken". Who said that? Joe Stalin? Adolf Hitler? Orwell's "Big Brother"? The Spanish Inquisition? Generalissimo Francisco Franco Bahamonde? None of those. It was Dr Colin Waine, chairman of Britain's National Obesity Forum. What a fine fellow!
*********************
7 March, 2008
Some Experts Doubt Obesity Epidemic
Go on, have another doughnut. According to some experts whose views are public health heresy, the jury is still out on how dangerous it is to be fat. "The obesity epidemic has absolutely been exaggerated," said Dr. Vincent Marks, emeritus professor of clinical biochemistry at the University of Surrey. Marks is among a minority of skeptics who doubt the severity of the obesity problem. They claim that the data about the dangers of obesity are mixed and there is little proof that being fat causes problems including high blood pressure, heart disease and cancer. Such views contradict nearly everything doctors have been saying for years.
Being fat has long been blamed for conditions like diabetes, which can lead to heart, kidney and nerve diseases. There is also increasing evidence that certain cancers may be linked to weight gain. "The evidence linking obesity to diabetes and cardiovascular disease is very strong," said Dr. James Hill, director of the Center for Human Nutrition at the University of Colorado. "Type two diabetes rarely happens in people who aren't obese."
But obesity contrarians say that there's no data proving why being fat - in itself - would be dangerous. "There's no good causal connection," said Eric Oliver, author of Fat Politics and a political science professor at the University of Chicago. Blaming obesity for diabetes and heart attacks, Oliver says, is like blaming lung cancer on bad breath rather than on smoking. Excess weight may actually be a red herring, Oliver says, since other factors like exercise, diet or genetic predispositions towards diseases are harder to measure than weight.
In addition to questioning the dangers of being fat, researchers like Marks also criticize oft-repeated alarmist projections about the rise in obesity - like the British government's warning that nearly half of Britain will be obese by 2050. Those simply aren't based on good evidence, they say. According to national health statistics released last month, from 1993 to 2006, "relatively little change" was noted in weight gain, with men and women gaining an average of about 4 kilograms (9 pounds). In children, no significant gains were recorded.
The main problem, obesity skeptics say, is that too many people are considered fat, with the obese and overweight often lumped together. "Being moderately plump is not a health disadvantage," Marks said. "Some overweight people may not look svelte, but they may be perfectly healthy." As defined by the World Health Organization, anyone with a body mass index above 25 is overweight, and anyone above 30 is obese. Most experts agree the distinctions are imperfect and somewhat arbitrary.
Moreover, Marks and others point to research showing the benefits of a few extra kilos (pounds). In 2005, Katherine Flegal of the United States' Centers for Disease Control and Prevention published a study in the Journal of the American Medical Association, finding that overweight people typically live longer than normal-weight people. More than a dozen other studies have come to the same conclusion.
Outrage ensued. Prominent health experts called the research flawed and worried that people would gleefully supersize their meals. "I think some experts found it disturbing that we actually said that overweight people have a lower death risk," Flegal said. In other research, Flegal and colleagues found there to be almost no link between death rates and weight. "The relationship between weight and disease and survival is very complex and we don't have a good handle on why some of these things are related and others are not," Flegal said. She suggested that being fat may help you survive some conditions, but not others.
Doctors have long struggled to explain the obesity paradox - the mystery that in certain conditions like heart attacks, fat patients often have better odds of surviving than thin people. Some experts hypothesize that fat peoples' hearts already work harder than those of thin people, thus giving them a natural edge when their bodies are stressed. "We don't want people to think it's ok to be heavier," said Hill. "But not everybody who gains weight is going to get heart disease or diabetes," he said.
Some obesity skeptics question the motives of experts who make dire predictions about obesity. With millions of dollars for obesity researchers, an industry of anti-fat drugs, and a boom in the number of doctors offering surgeries like stomach-stapling, the more fat people there are, the more profits there will be in selling them solutions.
Experts on both sides of the obesity debate have often criticized WHO's overweight and obesity measures, saying they are too low. When WHO defined the body mass index scores constituting normal, overweight and obese, they appeared to be the result of an independent expert committee convened by WHO. Yet the 1997 Geneva consultation was held jointly with the International Obesity Task Force, an advocacy group whose self-described mission is "to inform the world about the urgency of the (obesity) problem."
According to the task force's most recent available annual report, more than 70 percent of their funding came from Abbott Laboratories and F. Hoffman La-Roche, companies which make top-selling anti-fat pills. The task force remains one of Europe's most influential obesity advocacy groups and continues to work closely with WHO.
The blurred lines between pharmaceutical money and obesity groups have also caused concern in Britain. In 2006, one of the country's top obesity doctors quit the organization he founded to combat obesity, the National Obesity Forum, complaining that its goals had been skewed by drug money. "There's not a lot of money in trying to debunk obesity, but a huge amount in making sure it stays a big problem," said Patrick Basham, a professor of health care policy at Johns Hopkins University.
Still, while skeptics insist that obesity warnings must be taken with a grain of salt, nearly all agree that while a little bit of extra padding may not be too deadly, too much almost certainly is. "The vast majority of people who get labeled under the obesity epidemic are well under 300 pounds and probably are not facing big health consequences," Oliver said. "It's the morbidly obese people who should be worried."
Source
Snow eating now endangered kid pleasure

To the list of simple childhood pleasures whose safety has been questioned, add this: eating snow. A recent study found that snow - even in relatively pristine spots like Montana and the Yukon - contains large amounts of bacteria. Parents who warn their kids not to eat dirty snow (especially the yellow variety) are left wondering whether to stop them from tasting the new-fallen stuff, too, because of Pseudomonas syringae, bacteria that can cause diseases in bean and tomato plants.
But experts say there's no need to banish snow-eating along with dodgeball, unchaperoned trick-or-treating and riding a bike without a helmet. "It's a very ubiquitous bacteria that's everywhere," says Dr. Penelope Dennehy, a member of the American Academy of Pediatrics' committee on infectious diseases. "Basically, none of the food we eat is sterile. We eat bacteria all the time." Children practically bathe in bacteria when they go to the playground, and Dennehy says they won't get anything from snow that they wouldn't get from dirt. "We eat stuff that's covered with bacteria all the time, and for the most part it's killed in the stomach," says Dr. Joel Forman, a member of the pediatric academy's committee on environmental health. "Your stomach is a fantastic barrier against invasive bacteria because it's a very acidic environment."
There are exceptions. "Tiny kids on formula a lot of times don't have the acid in their stomachs," making them more vulnerable to bacteria in general, says Dr. Lynnette Mazur, a professor of pediatrics at the University of Texas Medical School. Also, Forman and Mazur say that Pseudomonas can be a threat to people with cystic fibrosis.
The study, published last week in the journal Science, didn't examine the effects on people. And experts say without further information, it is impossible to say what the bacteria could do to a child who eats extraordinary amounts. "I can say that I'm not aware of any clinical reports of children becoming ill from eating snow. And I looked," Forman says.
In any case, because of ordinary air pollution in snow, it's probably wise not to eat a lot of the stuff, pediatricians say. For parents in search of guidance, Mazur offers this: Licking a little snow off a glove is probably OK. "A meal of snow" is not.
Some parents say they are not going to worry about their kids eating snow that looks clean. "My snow-eating concerns are generally more of the dirt-urine variety," says Kristin Lang, 37, of Maplewood, N.J., whose 2-year-old son Charlie has swallowed his share of snow. "When I heard bacteria, at first I went 'eew,'" says Tricia Sweeney, a mother of three in Cornwall-on-Hudson, N.Y. But as long as the kids eat snow as it's falling, "I think it's OK. I tell them not to eat it if it's on the ground."
Source
****************
Just some problems with the "Obesity" war:
1). It tries to impose behavior change on everybody -- when most of those targeted are not obese and hence have no reason to change their behaviour. It is a form of punishing the innocent and the guilty alike. (It is also typical of Leftist thinking: Scorning the individual and capable of dealing with large groups only).
2). The longevity research all leads to the conclusion that it is people of MIDDLING weight who live longest -- not slim people. So the "epidemic" of obesity is in fact largely an "epidemic" of living longer.
3). It is total calorie intake that makes you fat -- not where you get your calories. Policies that attack only the source of the calories (e.g. "junk food") without addressing total calorie intake are hence pissing into the wind. People involuntarily deprived of their preferred calorie intake from one source are highly likely to seek and find their calories elsewhere.
4). So-called junk food is perfectly nutritious. A big Mac meal comprises meat, bread, salad and potatoes -- which is a mainstream Western diet. If that is bad then we are all in big trouble.
5). Food warriors demonize salt and fat. But we need a daily salt intake to counter salt-loss through perspiration and the research shows that people on salt-restricted diets die SOONER. And Eskimos eat huge amounts of fat with no apparent ill-effects. And the average home-cooked roast dinner has LOTS of fat. Will we ban roast dinners?
6). The foods restricted are often no more calorific than those permitted -- such as milk and fruit-juice drinks.
7). Tendency to weight is mostly genetic and is therefore not readily susceptible to voluntary behaviour change.
8). And when are we going to ban cheese? Cheese is a concentrated calorie bomb and has lots of that wicked animal fat in it too. Wouldn't we all be better off without it? And what about butter and margarine? They are just about pure fat. Surely they should be treated as contraband in kids' lunchboxes! [/sarcasm].
9). And how odd it is that we never hear of the huge American study which showed that women who eat lots of veggies have an INCREASED risk of stomach cancer? So the official recommendation to eat five lots of veggies every day might just be creating lots of cancer for the future! It's as plausible (i.e. not very) as all the other dietary "wisdom" we read about fat etc.
10). And will "this generation of Western children be the first in history to lead shorter lives than their parents did"? This is another anti-fat scare that emanates from a much-cited editorial in a prominent medical journal that said so. Yet this editorial offered no statistical basis for its opinion -- an opinion that flies directly in the face of the available evidence.
Even statistical correlations far stronger than anything found in medical research may disappear if more data is used. A remarkable example from Sociology:"The modern literature on hate crimes began with a remarkable 1933 book by Arthur Raper titled The Tragedy of Lynching. Raper assembled data on the number of lynchings each year in the South and on the price of an acre's yield of cotton. He calculated the correlation coefficient between the two series at -0.532. In other words, when the economy was doing well, the number of lynchings was lower.... In 2001, Donald Green, Laurence McFalls, and Jennifer Smith published a paper that demolished the alleged connection between economic conditions and lynchings in Raper's data. Raper had the misfortune of stopping his analysis in 1929. After the Great Depression hit, the price of cotton plummeted and economic conditions deteriorated, yet lynchings continued to fall. The correlation disappeared altogether when more years of data were added."So we must be sure to base our conclusions on ALL the data. But in medical research, data selectivity and the "overlooking" of discordant research findings is epidemic.
"What we should be doing is monitoring children from birth so we can detect any deviations from the norm at an early stage and action can be taken". Who said that? Joe Stalin? Adolf Hitler? Orwell's "Big Brother"? The Spanish Inquisition? Generalissimo Francisco Franco Bahamonde? None of those. It was Dr Colin Waine, chairman of Britain's National Obesity Forum. What a fine fellow!
*********************
6 March, 2008
WHAT HAPPENS WHEN OLDER WOMEN STOP TAKING HRT?
The headline on the article below is misleading. What it refers to is the controversial WHI study -- in which a clinical trial was stopped after old ladies on HRT pills seemed to be getting more cancer. Subsequent analyses, however concluded that the panic was unwarranted. So the claim that cancer risk "continues" is ill-informed. Any cancer risk shown in the original study was vanishingly small. See here and here for instance.
The panic reaction did however set the scene for another interesting study -- of what happens when women go off HRT. Are women who once took HRT more at risk than those on placebo? It was found that such women were at NO greater risk of heart events but did get more breast cancer (3.5% of the HRT group got cancer versus 2.7% for the non-HRT group). Clearly, however, the degree of risk was small in any case and the elevation of risk would be unlikely to be of much concern to most women. Taking ANY drug entails some risk of side effects and it is the balance between benefit and harm that rational users have to consider.
Of greater interest was the study of what happens when you consider ALL the illnesses that the old ladies concerned got. HRT therapy has some apparent favourable impacts on disease as well as adverse impacts. It was reported that the difference in disease incidence overall was quite minute (2.9% versus 2.4%). Once again, then, we see quite unjustified panic. Popular article followed by journal abstract below
Cancer risk continues even after women stop hormone treatment
Hormone replacement therapy continues to increase the risk of cancer even after a woman stops taking it, a study has shown. Three years after treatment ceased, the risk of breast cancer remained 27 per cent higher while risks of any type of cancer were 24 per cent higher. The findings, published in the Journal of the American Medical Association, imply that cancer risks persist, while other health risks such as blood clots and strokes - which are elevated while the women were taking the pills - returned to normal.
The results come from a follow-up to the Women's Health Initiative study, which gave warning in 2002 of cancer risks while taking HRT. After those findings were published and backed by results from the Million Women Study in 2003, about half the two million British women who had been taking HRT stopped. More recently, the health initiative study has been criticised for failing to break down the results by age. Among women in their fifties, defenders of HRT said, the risks were much smaller.
The new study, led by Gerardo Heiss, of the University of North Carolina, follows 15,730 women originally included in the trial, with an average age of 63. All had been randomised to take either the combined HRT pill (oestrogen plus progestagen, called progestin in the US) or a placebo.
In 2002, when researchers discovered an increased risk of breast cancer and heart and artery disease in women assigned to HRT, the trial was terminated. All the women were advised to stop taking the pills. The study looks at what happened in the following three years, up to 2005. At the end of that time the numbers of heart attacks, strokes and blood clots in women from both the active and placebo treatment groups were similar, showing that the risk of cardio-vascular disease had fallen substantially for former HRT users. While taking the treatment, the women had experienced a 29 per cent increased risk of heart attacks, a 41 per cent increased risk of strokes and nearly twice the normal risk of serious blood clots. These returned to normal after stopping.
But the increased risk of breast cancer remained at about the same level. During the follow-up study there were 63 more diagnoses of cancer among former HRT users than among women who did not have the treatment, or three per 1,000 participants per year. Marcia Stefanick, one of the study authors, from Stanford University, California, said: "The continued increased risk of breast cancer clearly plays a role in the increased overall risk of cancer, years after stopping long-term oestrogen plus progestin therapy, and it is important that we continue to follow these women." Leslie Ford, from the US National Institutes of Health, which funded the Women's Health Initiative, said: "The hormones' effects on breast cancer appear to linger. These findings reinforce the importance of women getting regular breast exams and mammograms even after they stop hormone therapy."
A summary of risks and benefits, called the "global index", was included in the results and covered outcomes for heart disease, invasive breast cancer, stroke, lung blood clots, cancer of the womb lining, bowel cancer, hip fracture and death. This overall measure showed an increased risk of 12 per cent for women taking HRT, which did not change after treatment stopped.
Michael Lauer, director of the National Heart Lung and Blood Institute at the US National Institutes of Health, said: "This study provides further evidence that five years of combination hormone therapy is harmful. All the accumulated risks do not simply disappear."
The advice from drug regulators in Britain is that HRT should be used for the control of symptoms of the menopause at the minimum effective dose and for the shortest possible time. That maximises the benefit and reduces the risks, since the evidence is that most of the damaging effects of HRT occur after the age of 60. In particular, HRT in younger women appears to cut heart attacks rather than increase them.
The new study does not attempt to break down the results by age so it is impossible to tell whether the persistent cancer risk is age-related. In the US, some researchers have linked a rapid fall in breast-cancer rates of 6.3 per cent in 2003 to the abandonment of HRT by so many women. The new trial fails to corroborate this claim because it contained too few women to detect a change of this order. Further follow-up was needed, the authors said.
Source
Health Risks and Benefits 3 Years After Stopping Randomized Treatment With Estrogen and Progestin
By Gerardo Heiss et al.
Context: The Women's Health Initiative (WHI) trial of estrogen plus progestin vs placebo was stopped early, after a mean 5.6 years of follow-up, because the overall health risks of hormone therapy exceeded its benefits.
Objective: To report health outcomes at 3 years (mean 2.4 years of follow-up) after the intervention was stopped.
Design, Setting, and Participants: The intervention phase was a double-blind, placebo-controlled, randomized trial of conjugated equine estrogens (CEE) 0.625 mg daily plus medroxyprogesterone acetate (MPA) 2.5 mg daily, in 16 608 women aged 50 through 79 years, recruited by 40 centers from 1993 to 1998. The postintervention phase commenced July 8, 2002, and included 15,730 women.
Main Outcome Measures: Semi-annual monitoring and outcomes ascertainment continued per trial protocol. The primary end points were coronary heart disease and invasive breast cancer. A global index summarizing the balance of risks and benefits included the 2 primary end points plus stroke, pulmonary embolism, endometrial cancer, colorectal cancer, hip fracture, and death due to other causes.
Results: The risk of cardiovascular events after the intervention was comparable by initial randomized assignments, 1.97% (annualized rate) in the CEE plus MPA (343 events) and 1.91% in the placebo group (323 events). A greater risk of malignancies occurred in the CEE plus MPA than in the placebo group (1.56% [n = 281] vs 1.26% [n = 218]; hazard ratio [HR], 1.24; 95% confidence interval [CI], 1.04-1.48). More breast cancers were diagnosed in women who had been randomly assigned to receive CEE plus MPA vs placebo (0.42% [n = 79] vs 0.33% [n = 60]; HR, 1.27; 95% CI, 0.91-1.78) with a modest trend toward a lower HR during the follow-up after the intervention. All-cause mortality was somewhat higher in the CEE plus MPA than in the placebo group (1.20% [n = 233] vs 1.06% [n = 196]; HR, 1.15; 95% CI, 0.95-1.39). The global index of risks and benefits was unchanged from randomization through March 31, 2005 (HR, 1.12; 95% CI, 1.03-1.21), indicating that the risks of CEE plus MPA exceed the benefits for chronic disease prevention.
Conclusions: The increased cardiovascular risks in the women assigned to CEE plus MPA during the intervention period were not observed after the intervention. A greater risk of fatal and nonfatal malignancies occurred after the intervention in the CEE plus MPA group and the global risk index was 12% higher in women randomly assigned to receive CEE plus MPA compared with placebo.
JAMA. 2008;299(9):1036-1045
DOES PSYCHOLOGY ALONE BENEFIT DEPRESSED PEOPLE?
I commented recently on the inconclusive study of Prozac and similar drugs which showed that in some groups the drugs helped a lot but in others the drugs seemed to help not at all. I concluded that the real challenge of the finding lay in sorting out which patients would be in the benefited group.
The study below gets an opportunistic boost off that finding. "If the pills don't work, what does?" is their question. It is however a most incompetent study with no placebo group so should be disregarded. One might remark in fact that the apparent benefits reported for psychological therapy were rather what one would expect from a placebo effect. Popular article followed by journal abstract below
Depressed teenagers whose medication is not working should switch medications and start cognitive behavioural therapy (CBT), a specific type of psychotherapy, according to a new study in the Journal of the American Medical Association. The study involved 334 patients with major depressive disorder, aged 12 to 18 years. All of the participants had taken an antidepressant called an SSRI (selective serotonin re-uptake inhibitor) for two months, with no improvement in symptoms. For the next 12 weeks, they were divided into four groups. The first group switched to a different SSRI (paroxetine, citalopram or fluoxetine); the second group switched to a different SSRI and were given CBT, while the third group switched to venlafaxine -- a different type of antidepressant called an SNRI (serotonin and noradrenaline reuptake inhibitor) -- and the fourth group switched to venlafaxine and were also given CBT. Of those who switched to a combination of medication and CBT, 55 per cent showed improvement, regardless of the drug type. Only 41 per cent of those who simply switched medication showed an improvement in symptoms after 12 weeks.
Source
Switching to Another SSRI or to Venlafaxine With or Without Cognitive Behavioral Therapy for Adolescents With SSRI-Resistant Depression
By David Brent et al.
Context: Only about 60% of adolescents with depression will show an adequate clinical response to an initial treatment trial with a selective serotonin reuptake inhibitor (SSRI). There are no data to guide clinicians on subsequent treatment strategy.
Objective: To evaluate the relative efficacy of 4 treatment strategies in adolescents who continued to have depression despite adequate initial treatment with an SSRI.
Design, Setting, and Participants: Randomized controlled trial of a clinical sample of 334 patients aged 12 to 18 years with a primary diagnosis of major depressive disorder that had not responded to a 2-month initial treatment with an SSRI, conducted at 6 US academic and community clinics from 2000-2006.
Interventions Twelve weeks of: (1) switch to a second, different SSRI (paroxetine, citalopram, or fluoxetine, 20-40 mg); (2) switch to a different SSRI plus cognitive behavioral therapy; (3) switch to venlafaxine (150-225 mg); or (4) switch to venlafaxine plus cognitive behavioral therapy.
Main Outcome Measures: Clinical Global Impressions-Improvement score of 2 or less (much or very much improved) and a decrease of at least 50% in the Children's Depression Rating Scale-Revised (CDRS-R); and change in CDRS-R over time.
Results: Cognitive behavioral therapy plus a switch to either medication regimen showed a higher response rate (54.8%; 95% confidence interval [CI], 47%-62%) than a medication switch alone (40.5%; 95% CI, 33%-48%; P = .009), but there was no difference in response rate between venlafaxine and a second SSRI (48.2%; 95% CI, 41%-56% vs 47.0%; 95% CI, 40%-55%; P = .83). There were no differential treatment effects on change in the CDRS-R, self-rated depressive symptoms, suicidal ideation, or on the rate of harm-related or any other adverse events. There was a greater increase in diastolic blood pressure and pulse and more frequent occurrence of skin problems during venlafaxine than SSRI treatment.
Conclusions: For adolescents with depression not responding to an adequate initial treatment with an SSRI, the combination of cognitive behavioral therapy and a switch to another antidepressant resulted in a higher rate of clinical response than did a medication switch alone. However, a switch to another SSRI was just as efficacious as a switch to venlafaxine and resulted in fewer adverse effects.
JAMA. 2008;299(8):901-913.
****************
Just some problems with the "Obesity" war:
1). It tries to impose behavior change on everybody -- when most of those targeted are not obese and hence have no reason to change their behaviour. It is a form of punishing the innocent and the guilty alike. (It is also typical of Leftist thinking: Scorning the individual and capable of dealing with large groups only).
2). The longevity research all leads to the conclusion that it is people of MIDDLING weight who live longest -- not slim people. So the "epidemic" of obesity is in fact largely an "epidemic" of living longer.
3). It is total calorie intake that makes you fat -- not where you get your calories. Policies that attack only the source of the calories (e.g. "junk food") without addressing total calorie intake are hence pissing into the wind. People involuntarily deprived of their preferred calorie intake from one source are highly likely to seek and find their calories elsewhere.
4). So-called junk food is perfectly nutritious. A big Mac meal comprises meat, bread, salad and potatoes -- which is a mainstream Western diet. If that is bad then we are all in big trouble.
5). Food warriors demonize salt and fat. But we need a daily salt intake to counter salt-loss through perspiration and the research shows that people on salt-restricted diets die SOONER. And Eskimos eat huge amounts of fat with no apparent ill-effects. And the average home-cooked roast dinner has LOTS of fat. Will we ban roast dinners?
6). The foods restricted are often no more calorific than those permitted -- such as milk and fruit-juice drinks.
7). Tendency to weight is mostly genetic and is therefore not readily susceptible to voluntary behaviour change.
8). And when are we going to ban cheese? Cheese is a concentrated calorie bomb and has lots of that wicked animal fat in it too. Wouldn't we all be better off without it? And what about butter and margarine? They are just about pure fat. Surely they should be treated as contraband in kids' lunchboxes! [/sarcasm].
9). And how odd it is that we never hear of the huge American study which showed that women who eat lots of veggies have an INCREASED risk of stomach cancer? So the official recommendation to eat five lots of veggies every day might just be creating lots of cancer for the future! It's as plausible (i.e. not very) as all the other dietary "wisdom" we read about fat etc.
10). And will "this generation of Western children be the first in history to lead shorter lives than their parents did"? This is another anti-fat scare that emanates from a much-cited editorial in a prominent medical journal that said so. Yet this editorial offered no statistical basis for its opinion -- an opinion that flies directly in the face of the available evidence.
Even statistical correlations far stronger than anything found in medical research may disappear if more data is used. A remarkable example from Sociology:"The modern literature on hate crimes began with a remarkable 1933 book by Arthur Raper titled The Tragedy of Lynching. Raper assembled data on the number of lynchings each year in the South and on the price of an acre's yield of cotton. He calculated the correlation coefficient between the two series at -0.532. In other words, when the economy was doing well, the number of lynchings was lower.... In 2001, Donald Green, Laurence McFalls, and Jennifer Smith published a paper that demolished the alleged connection between economic conditions and lynchings in Raper's data. Raper had the misfortune of stopping his analysis in 1929. After the Great Depression hit, the price of cotton plummeted and economic conditions deteriorated, yet lynchings continued to fall. The correlation disappeared altogether when more years of data were added."So we must be sure to base our conclusions on ALL the data. But in medical research, data selectivity and the "overlooking" of discordant research findings is epidemic.
"What we should be doing is monitoring children from birth so we can detect any deviations from the norm at an early stage and action can be taken". Who said that? Joe Stalin? Adolf Hitler? Orwell's "Big Brother"? The Spanish Inquisition? Generalissimo Francisco Franco Bahamonde? None of those. It was Dr Colin Waine, chairman of Britain's National Obesity Forum. What a fine fellow!
*********************
5 March, 2008
Study links heavy cell phone use to cancer
Another stupid epidemiological study relying on self-reports. If they had asked enough questions, they would probably have found several correlates of tumor incidence -- all by chance
Scientists claim to have found a link between heavy cell phone usage and cancer of the salivary gland. The researchers suggest people use handsfree cell phones to avoid a risk.
The findings by Siegal Sadetzki, an epidemiologist at Tel Aviv University in Israel, and colleagues appear in the Feb. 15 issue of the American Journal of Epidemiology. The group found that heavy cell phone users faced a higher risk of both benign and malignant tumors in the gland.
People who used a cell phone heavily on the side of the head where the tumor developed were found to have an about 50 percent higher risk for developing a tumor of the main salivary gland, or parotid, compared to noncell phone users, the researchers wrote.
The study was done on Israelis, which is a key because Israelis adopted cell phone technology early and use it heavily, Sadetzki said. Thus the exposure to phone radiation found in this study was higher than in previous studies."This unique population has given us an indication that cell phone use is associated with cancer," added Sadetzki.
The study investigated nearly 500 people diagnosed with salivary gland tumors, and compared them to 1,300 healthy subjects. Participants were asked to detail how often and how long they typically talked on cell phones. The study also found an increased risk of cancer for heavy users who lived in rural areas. Because there are fewer antennas, cell phones in rural areas need to emit more radiation to communicate effectively.
Sadetzki predicts that, over time, the greatest effects will be found in heavy users and children. Risks from cell phones have been hard to prove, mainly due to the long time it takes cancer to develop, she said. "This technology is here to stay," Sadetzki said. "I believe precautions should be taken in order to diminish the exposure." She recommends people use handsfree devices, and hold the phone away from one's body. Less frequent and shorter calls are also preferable, she added.
Children may be more susceptible, so parents should limit youngsters' cell phone use and insist they use speakers or handsfree devices, she added. "Some technology that we use today carries a risk. The question is not if we use it, but how we use it."
Precisely how cell phones could affect the body is unclear, but a recent Finnish Radiation and Nuclear Safety Authority study found their radiation might subtly change the biochemical makeup of skin. That research appeared in the Feb. 11 online issue of the journal BMC Genomics.
Source
Insurers cash in on "obesity" hysteria
It's actually people of middling weight who live longest so this is just a scam
A "Fat tax" is being imposed on the obese, with life insurance firms charging at least 50 per cent more on their premiums. The increased charge can be as much as 300 per cent if obese applicants fall into other high-risk health categories, such as being a smoker or having previous medical conditions. All major insurance companies have introduced the policy, according to brokers.
Lifebroker Financial Assurance, Australia's leading online life insurance broker, told The Sunday Telegraph that overweight people should expect to pay higher premiums. Chantelle Pain, insurance consultant with the firm, said: "Some insurers are more lenient than others, but the premium which obese people pay ranges from 50 per cent extra. "Being significantly overweight means you are at greater risk of contracting certain diseases. It is the same as increasing a smoker's premium or someone who has previous medical conditions."
A body mass index (BMI) of 30 or more is attracting the price hike. This is assessed when you fill out an application form that requires you to provide your personal details including height and weight. A BMI of 20 to 25 for adults is considered healthy, but some doctors believe a BMI figure may not always be an accurate measure of health, as athletes often have a high weight-to-height due to the muscles built up for their sport.
For a healthy, non-smoking 55-year-old man with no weight problems, life insurance should cost about $1700 a year for $500,000 of cover. If he were obese, the annual premium could cost an extra $850.
While agreeing "there has to be consequences for lifestyle choices", Dr Steve Hambleton, a spokesman for the Australian Medical Association in Queensland, said companies were simply cashing in on the country's obesity crisis. "It seems rather opportunistic of insurers to be adding as much as 50 per cent on simply because someone is obese," he said.
Source
****************
Just some problems with the "Obesity" war:
1). It tries to impose behavior change on everybody -- when most of those targeted are not obese and hence have no reason to change their behaviour. It is a form of punishing the innocent and the guilty alike. (It is also typical of Leftist thinking: Scorning the individual and capable of dealing with large groups only).
2). The longevity research all leads to the conclusion that it is people of MIDDLING weight who live longest -- not slim people. So the "epidemic" of obesity is in fact largely an "epidemic" of living longer.
3). It is total calorie intake that makes you fat -- not where you get your calories. Policies that attack only the source of the calories (e.g. "junk food") without addressing total calorie intake are hence pissing into the wind. People involuntarily deprived of their preferred calorie intake from one source are highly likely to seek and find their calories elsewhere.
4). So-called junk food is perfectly nutritious. A big Mac meal comprises meat, bread, salad and potatoes -- which is a mainstream Western diet. If that is bad then we are all in big trouble.
5). Food warriors demonize salt and fat. But we need a daily salt intake to counter salt-loss through perspiration and the research shows that people on salt-restricted diets die SOONER. And Eskimos eat huge amounts of fat with no apparent ill-effects. And the average home-cooked roast dinner has LOTS of fat. Will we ban roast dinners?
6). The foods restricted are often no more calorific than those permitted -- such as milk and fruit-juice drinks.
7). Tendency to weight is mostly genetic and is therefore not readily susceptible to voluntary behaviour change.
8). And when are we going to ban cheese? Cheese is a concentrated calorie bomb and has lots of that wicked animal fat in it too. Wouldn't we all be better off without it? And what about butter and margarine? They are just about pure fat. Surely they should be treated as contraband in kids' lunchboxes! [/sarcasm].
9). And how odd it is that we never hear of the huge American study which showed that women who eat lots of veggies have an INCREASED risk of stomach cancer? So the official recommendation to eat five lots of veggies every day might just be creating lots of cancer for the future! It's as plausible (i.e. not very) as all the other dietary "wisdom" we read about fat etc.
10). And will "this generation of Western children be the first in history to lead shorter lives than their parents did"? This is another anti-fat scare that emanates from a much-cited editorial in a prominent medical journal that said so. Yet this editorial offered no statistical basis for its opinion -- an opinion that flies directly in the face of the available evidence.
Even statistical correlations far stronger than anything found in medical research may disappear if more data is used. A remarkable example from Sociology:"The modern literature on hate crimes began with a remarkable 1933 book by Arthur Raper titled The Tragedy of Lynching. Raper assembled data on the number of lynchings each year in the South and on the price of an acre's yield of cotton. He calculated the correlation coefficient between the two series at -0.532. In other words, when the economy was doing well, the number of lynchings was lower.... In 2001, Donald Green, Laurence McFalls, and Jennifer Smith published a paper that demolished the alleged connection between economic conditions and lynchings in Raper's data. Raper had the misfortune of stopping his analysis in 1929. After the Great Depression hit, the price of cotton plummeted and economic conditions deteriorated, yet lynchings continued to fall. The correlation disappeared altogether when more years of data were added."So we must be sure to base our conclusions on ALL the data. But in medical research, data selectivity and the "overlooking" of discordant research findings is epidemic.
"What we should be doing is monitoring children from birth so we can detect any deviations from the norm at an early stage and action can be taken". Who said that? Joe Stalin? Adolf Hitler? Orwell's "Big Brother"? The Spanish Inquisition? Generalissimo Francisco Franco Bahamonde? None of those. It was Dr Colin Waine, chairman of Britain's National Obesity Forum. What a fine fellow!
*********************
4 March, 2008
Does obesity cause diabetes?
That obesity causes diabetes is almost a mantra. I think I see it claimed or implied at least once a day. See the article immediately below this one, for instance. So I decided to look at the evidence behind the claim. I looked at what appear to be the two most cited articles on the question -- by Seidell and by Mokdad et al..
Neither article goes any where near proving the claim. Seidell, in fact, notes the differing relationship between weight and diabetes in Asia versus the West and makes the entirely sensible observation that the two things are "common consequences of changing lifestyles" -- NOT directly linked, in other words. Both, for instance, could be a consequence of (say) reduced exercise.
And the Mokdad article is quite naive. It shows that fatties are more likely to have diabetes but again enables no causal inferences. Additionally, it does not allow for the curvilearity that is known to feature in relationships with obesity. In other words, it combines moderately overweight people with grossly overweight people -- which fies in the face of the fact that it is people of middling weight who live longest. It could be just the real fatties who tend to get diabetes at an accelerated rate.
And genetic effects are, of course, not mentioned anywhere, despite all we know (and have known for a long time) about the genetic influence on body weight. It could be that a genetic difference causes both diabetes AND a larger fat mass. So even severe dieting would not chase that pesky diabetes-causing gene away.
The fact that prevalence of diabetes has been increasing would seem at first to discount a genetic influence but it does not, of course. Many genetic influences need environmental "triggers" to become dominant and we just don't know what environmental triggers might have come to the fore in recent years. How about increased crime causing both stress and overeating as a response to stress? Who knows?
As far as I can see, then, the alleged effect of fat on diabetes is just a guess. Ho hum! Just another instance of crap medical "wisdom".
I wonder do pigs get diabetes? Fat pigs are a byword. And pigs are a pretty good animal model for human beings. Pig tissue is even used for direct implantation into human hearts! Rodent models always have dubious generalizability but I think I would believe a double-blind study with pigs.
So, you see, I am not like those (such as the Global Warmists) for whom no evidence will count. I have just specified precisely what evidence would convince me. And nor would the evidence concerned be hard to gather. You might even get some good bacon at the end of it! Yum!
Jungle frog’s anti-infection agent may help millions of diabetics
A nocturnal frog that dwells in the ponds and lagoons of the Amazon could prove to be an unlikely lifesaver for millions of people suffering from diabetes, researchers say. The South American “paradoxical frog” (Pseudis paradoxa) owes its name to an uncanny ability to shrink as it grows older. Scientists studying the properties of its slimy skin have found a substance that can stimulate the release of insulin, the vital hormone that is deficient in sufferers from diabetes.
Scientists have made an artificial copy of the peptide, a protein-building block that protects the frog from infection, and have suggested that it could be used to boost insulin production in people with Type 2 diabetes. In laboratory tests, researchers found that the paradoxical frog’s peptide, known as pseudin-2, increased release of insulin in cultured cells by 50 per cent. However, more work must be carried out before the therapy is ready to be tested on human patients.
Currently there are 2.3 million diagnosed sufferers from diabetes in the UK, most of whom have the Type 2 form of the disease. Usually occurring in middle age, Type 2 diabetes is strongly associated with lifestyle factors such as obesity and develops because the body does not produce enough insulin or becomes resistant to the concentrations available.
The joint team from the University of Ulster in Northern Ireland and United Arab Emirates University believe that a synthetic version of pseudin-2 could join a new class of medicines, called incretin mimetics, that help diabetics to control their condition when dietary changes or other medicines have failed.
The skin secretions of frogs and other amphibians are being investigated as a rich source of biological agents that may lead to new drugs. Byetta, a diabetes drug based on the saliva of an endangered lizard, the Gila monster of North America, is already available in the UK. But scientists believe that the frog’s secretions could be even more effective. Paradoxical frogs are one of the few animals whose young are bigger than their parents, with tadpoles growing up to 27cm (11in) in length while the mature frogs are only about 4cm long.
Yasser Abdel-Wahab, senior lecturer in biomedical sciences at the University of Ulster, said that the chemistry of amphibian peptides was very similar to that of some mammalian counterparts that help to regulate blood sugar. He studied samples from several different species of frog before finding the desired effect, he said. “We are at an exciting stage with this research,” he said. “We have tested a more potent synthetic version of the pseudin-2 peptide and have found that it has the potential for development into a compound for the treatment of Type 2 diabetes. Now we need to take this a step further and put our work into practice to try and help people with Type 2 diabetes. “More research is needed, but there is a growing body of work around natural anti-diabetic drug discovery that is already yielding fascinating results.” Further details of the research will be presented today at the Diabetes UK Annual Professional Conference in Glasgow.
Source
****************
Just some problems with the "Obesity" war:
1). It tries to impose behavior change on everybody -- when most of those targeted are not obese and hence have no reason to change their behaviour. It is a form of punishing the innocent and the guilty alike. (It is also typical of Leftist thinking: Scorning the individual and capable of dealing with large groups only).
2). The longevity research all leads to the conclusion that it is people of MIDDLING weight who live longest -- not slim people. So the "epidemic" of obesity is in fact largely an "epidemic" of living longer.
3). It is total calorie intake that makes you fat -- not where you get your calories. Policies that attack only the source of the calories (e.g. "junk food") without addressing total calorie intake are hence pissing into the wind. People involuntarily deprived of their preferred calorie intake from one source are highly likely to seek and find their calories elsewhere.
4). So-called junk food is perfectly nutritious. A big Mac meal comprises meat, bread, salad and potatoes -- which is a mainstream Western diet. If that is bad then we are all in big trouble.
5). Food warriors demonize salt and fat. But we need a daily salt intake to counter salt-loss through perspiration and the research shows that people on salt-restricted diets die SOONER. And Eskimos eat huge amounts of fat with no apparent ill-effects. And the average home-cooked roast dinner has LOTS of fat. Will we ban roast dinners?
6). The foods restricted are often no more calorific than those permitted -- such as milk and fruit-juice drinks.
7). Tendency to weight is mostly genetic and is therefore not readily susceptible to voluntary behaviour change.
8). And when are we going to ban cheese? Cheese is a concentrated calorie bomb and has lots of that wicked animal fat in it too. Wouldn't we all be better off without it? And what about butter and margarine? They are just about pure fat. Surely they should be treated as contraband in kids' lunchboxes! [/sarcasm].
9). And how odd it is that we never hear of the huge American study which showed that women who eat lots of veggies have an INCREASED risk of stomach cancer? So the official recommendation to eat five lots of veggies every day might just be creating lots of cancer for the future! It's as plausible (i.e. not very) as all the other dietary "wisdom" we read about fat etc.
10). And will "this generation of Western children be the first in history to lead shorter lives than their parents did"? This is another anti-fat scare that emanates from a much-cited editorial in a prominent medical journal that said so. Yet this editorial offered no statistical basis for its opinion -- an opinion that flies directly in the face of the available evidence.
Even statistical correlations far stronger than anything found in medical research may disappear if more data is used. A remarkable example from Sociology:"The modern literature on hate crimes began with a remarkable 1933 book by Arthur Raper titled The Tragedy of Lynching. Raper assembled data on the number of lynchings each year in the South and on the price of an acre's yield of cotton. He calculated the correlation coefficient between the two series at -0.532. In other words, when the economy was doing well, the number of lynchings was lower.... In 2001, Donald Green, Laurence McFalls, and Jennifer Smith published a paper that demolished the alleged connection between economic conditions and lynchings in Raper's data. Raper had the misfortune of stopping his analysis in 1929. After the Great Depression hit, the price of cotton plummeted and economic conditions deteriorated, yet lynchings continued to fall. The correlation disappeared altogether when more years of data were added."So we must be sure to base our conclusions on ALL the data. But in medical research, data selectivity and the "overlooking" of discordant research findings is epidemic.
"What we should be doing is monitoring children from birth so we can detect any deviations from the norm at an early stage and action can be taken". Who said that? Joe Stalin? Adolf Hitler? Orwell's "Big Brother"? The Spanish Inquisition? Generalissimo Francisco Franco Bahamonde? None of those. It was Dr Colin Waine, chairman of Britain's National Obesity Forum. What a fine fellow!
*********************
3 March, 2008
Spanking may lead to sexual problems later (?)
Out of the zillions of studies on corporal punishment, the guy apparently found only FOUR that supported his prejudices! And three of those are unpublished! What about all the other studies? The guy is just a missionary, not a scientist
Children whose parents spank them or otherwise inflict physical punishment may be more likely to have sexual problems later, according to research to be presented Thursday to the American Psychological Association. The analysis of four studies by Murray Straus, co-director of the Family Research Laboratory at the University of New Hampshire-Durham, suggests that children whose parents spanked, slapped, hit or threw objects at them may have a greater chance of physically or verbally coercing a sexual partner, engaging in risky sexual behavior or engaging in masochistic sex, including sexual arousal by spanking. "It increases the chances of sexual problems," though "it's not a one-to-one causation," Straus says.
Elizabeth Gershoff, an assistant professor of social work at the University of Michigan-Ann Arbor, who reviewed 80 years of spanking research in 2002 in the APA's Psychological Bulletin, says Straus' work appears to be the first to link spanking with sexual problems. Gershoff says that though many children have been spanked (85% in one 2007 survey), problems may depend on how they process the spanking. "They may internalize that to mean that in loving relationships sometimes there's pain or physical aggression," she says. Another possible lesson is that "whoever is stronger and has more power can overpower the other person and use physical aggression to control the other person's behavior."
But linking sexual problems with spanking is a "big leap," says human-sexuality researcher John DeLamater of the University of Wisconsin. "It's probably one of many elements that might contribute to sex problems or risky sex, but it's a long leap."
Most children who are spanked escape from long-term harm, says Straus, 81, a sociology professor who says he occasionally spanked his own children but later became a staunch critic of spanking. His work on violence in families is regarded as landmark research. He is scheduled to present the studies today at the psychological association's Summit on Violence and Abuse in Relationships in Bethesda, Md. Three are yet unpublished; one has been submitted to a journal. He plans to include two in a book this year. The fourth was included in a 1994 book.
The two most recent studies examine sexual coercion and risky practices among 14,252 college students between 2001 and 2006. The third study, of 440 high school students from New Hampshire, examined risky sex, such as premarital sex without a condom. The fourth study, of 207 students from the Northeast, focused on masochistic sex. In each case, Straus found that those who had experienced corporal punishment had increased probability of coercing sex, risky sex or masochistic sex.
The literature on effectiveness of spanking to correct behavior is still "very mixed," says Robert Larzelere of Oklahoma State University, who has studied parents' disciplinary methods. "Like any discipline tactic, it depends on how it's used," he says.
Source
If you think British food is bad, wait until you see British army food
Prince Harry returned yesterday from Afghanistan clearly unbowed by the threat of serious injury, kidnapping or death from a Taliban attack. But he admitted that sinking, defeated feeling when faced with some of the dismal army food. Harry said: "Rations are miserable. I've been on rations now for, I can't remember how long. The guys here [in Afghanistan] have been on rations even longer than I have. They're fed-up with it."
Responding to the suggestion that Jamie Oliver could be drafted in to help boost morale with some ration recipes, he said: "Yeah, Jamie, please. Bangers and mash with gravy, in a bag, would be brilliant. I don't think you can screw that up. I'm sure someone would manage to, but bangers and mash with gravy in a bag would be awesome." Harry, who typically prefers Big Macs, spent weeks living on rations while operating around Musa Qala, the former Taliban stronghold. "There are people out in the villages who have got less stuff than us, so I suppose we should be happy with a corned beef hash," he said.
The prince has, however, broadened his culinary experiences in Afghanistan - eating goat curry with a unit of Gurkhas. "Everyone is well looked after here by the Gurkhas, the food is fantastic - goat curries, chicken curries . . . it's good fun." The Gurkhas praised Harry for his good manners, noting how he would visit the camp kitchen after every meal to thank the cook. "We are very lucky to have a prince on our team working with us," said Captain Yambahadur Rana. "He's getting on very well with our boys. He has even started learning a few Gurkha words."
The prince's culinary experiences were broadened further when he join Fijian troops on manoeuvres in the Afghan desert. Their rudimentary breakfast entailed blending butter and jam in a tub and then spreading it on a wholemeal biscuit.
Source
****************
Just some problems with the "Obesity" war:
1). It tries to impose behavior change on everybody -- when most of those targeted are not obese and hence have no reason to change their behaviour. It is a form of punishing the innocent and the guilty alike. (It is also typical of Leftist thinking: Scorning the individual and capable of dealing with large groups only).
2). The longevity research all leads to the conclusion that it is people of MIDDLING weight who live longest -- not slim people. So the "epidemic" of obesity is in fact largely an "epidemic" of living longer.
3). It is total calorie intake that makes you fat -- not where you get your calories. Policies that attack only the source of the calories (e.g. "junk food") without addressing total calorie intake are hence pissing into the wind. People involuntarily deprived of their preferred calorie intake from one source are highly likely to seek and find their calories elsewhere.
4). So-called junk food is perfectly nutritious. A big Mac meal comprises meat, bread, salad and potatoes -- which is a mainstream Western diet. If that is bad then we are all in big trouble.
5). Food warriors demonize salt and fat. But we need a daily salt intake to counter salt-loss through perspiration and the research shows that people on salt-restricted diets die SOONER. And Eskimos eat huge amounts of fat with no apparent ill-effects. And the average home-cooked roast dinner has LOTS of fat. Will we ban roast dinners?
6). The foods restricted are often no more calorific than those permitted -- such as milk and fruit-juice drinks.
7). Tendency to weight is mostly genetic and is therefore not readily susceptible to voluntary behaviour change.
8). And when are we going to ban cheese? Cheese is a concentrated calorie bomb and has lots of that wicked animal fat in it too. Wouldn't we all be better off without it? And what about butter and margarine? They are just about pure fat. Surely they should be treated as contraband in kids' lunchboxes! [/sarcasm].
9). And how odd it is that we never hear of the huge American study which showed that women who eat lots of veggies have an INCREASED risk of stomach cancer? So the official recommendation to eat five lots of veggies every day might just be creating lots of cancer for the future! It's as plausible (i.e. not very) as all the other dietary "wisdom" we read about fat etc.
10). And will "this generation of Western children be the first in history to lead shorter lives than their parents did"? This is another anti-fat scare that emanates from a much-cited editorial in a prominent medical journal that said so. Yet this editorial offered no statistical basis for its opinion -- an opinion that flies directly in the face of the available evidence.
Even statistical correlations far stronger than anything found in medical research may disappear if more data is used. A remarkable example from Sociology:"The modern literature on hate crimes began with a remarkable 1933 book by Arthur Raper titled The Tragedy of Lynching. Raper assembled data on the number of lynchings each year in the South and on the price of an acre's yield of cotton. He calculated the correlation coefficient between the two series at -0.532. In other words, when the economy was doing well, the number of lynchings was lower.... In 2001, Donald Green, Laurence McFalls, and Jennifer Smith published a paper that demolished the alleged connection between economic conditions and lynchings in Raper's data. Raper had the misfortune of stopping his analysis in 1929. After the Great Depression hit, the price of cotton plummeted and economic conditions deteriorated, yet lynchings continued to fall. The correlation disappeared altogether when more years of data were added."So we must be sure to base our conclusions on ALL the data. But in medical research, data selectivity and the "overlooking" of discordant research findings is epidemic.
"What we should be doing is monitoring children from birth so we can detect any deviations from the norm at an early stage and action can be taken". Who said that? Joe Stalin? Adolf Hitler? Orwell's "Big Brother"? The Spanish Inquisition? Generalissimo Francisco Franco Bahamonde? None of those. It was Dr Colin Waine, chairman of Britain's National Obesity Forum. What a fine fellow!
*********************
2 March, 2008
Now vitamin E is bad for you
But hey! Isn't it one of those marvellous "antioxidants"? Pesky! Note that Vitamin D has also recently been shown to be bad for you. Note also here, where antioxidants generally were found to be BAD for you. So sad for all the credulous pill-poppers!
People who take daily supplements of vitamin E have a higher risk of developing lung cancer, according to one of the largest studies into vitamins and health ever attempted. Doctors monitored the wellbeing of more than 77,000 men and women over a four-year period and found that a range of vitamins failed to protect against lung cancer, while vitamin E slightly increased the risk of developing the disease. The study suggested that taking 400mg of vitamin E for 10 years increases the risk of lung cancer by 28%. Taking 100mg of the vitamin each day raised the risk of disease by 7%.
According to Cancer Research UK, the lifetime risk of developing lung cancer is roughly 8% for men and 4% for women. An increase of 28% in that background risk would raise a man's risk to 10% and a woman's to 5%.
A team led by Christopher Slatore at the University of Washington in Seattle looked at 77,126 people aged between 50 and 76 years old who were taking part in a vitamins and lifestyle study called Vital. By following the patients over several years, they were able to link their risk of lung cancer with previous and ongoing vitamin usage.
Unsurprisingly, the doctors found that lung cancer was strongly correlated with smoking, a family history of the disease and increasing age, but were surprised to find a slight but significant rise in lung cancer linked to vitamin E. The effect was most prominent in current smokers.
People who took multivitamins, vitamin C or folate supplements had a risk of lung cancer similar to those who did not take supplements, according to the study, which appears in the American Journal of Respiratory and Critical Care Medicine. "Our results should prompt clinicians to counsel patients that these supplements are unlikely to reduce the risk of lung cancer and may be detrimental," Slatore said.
In an accompanying editorial, Tim Byers at the University of Colorado School of Medicine says that many people use vitamins pills as a substitute for a healthy diet, but he said other compounds in fresh fruit and vegetables are also important. "Fruits contain not only vitamins but also many hundreds of other phytochemical compounds whose functions are not well understood," he writes.
Henry Scowcroft, senior science information officer at Cancer Research UK, said: "The jury's still very much out on whether vitamin and mineral supplements can affect cancer risk. Some studies suggest a benefit, but many others show no effect and some, like this one, suggest they may even increase risk. "Research repeatedly shows that a healthy, balanced diet [And how do we define "balanced"?] can reduce your risk of some cancers while giving you all the vitamins you need. And quitting smoking remains the most effective way to avoid many cancers. There's no diet or vitamin supplement that could ever counter the toxic effects of cigarette smoke."
The charity added: "Supplements do not substitute for a healthy diet, although some people may be advised to take them at certain times in their lives. For example, doctors may advise women who are planning to have a baby to take a daily 400-microgram supplement of folic acid. And dark-skinned or elderly people may need to take vitamin D supplements since they need more sun exposure than other people to make enough vitamin D."
Source
****************
Just some problems with the "Obesity" war:
1). It tries to impose behavior change on everybody -- when most of those targeted are not obese and hence have no reason to change their behaviour. It is a form of punishing the innocent and the guilty alike. (It is also typical of Leftist thinking: Scorning the individual and capable of dealing with large groups only).
2). The longevity research all leads to the conclusion that it is people of MIDDLING weight who live longest -- not slim people. So the "epidemic" of obesity is in fact largely an "epidemic" of living longer.
3). It is total calorie intake that makes you fat -- not where you get your calories. Policies that attack only the source of the calories (e.g. "junk food") without addressing total calorie intake are hence pissing into the wind. People involuntarily deprived of their preferred calorie intake from one source are highly likely to seek and find their calories elsewhere.
4). So-called junk food is perfectly nutritious. A big Mac meal comprises meat, bread, salad and potatoes -- which is a mainstream Western diet. If that is bad then we are all in big trouble.
5). Food warriors demonize salt and fat. But we need a daily salt intake to counter salt-loss through perspiration and the research shows that people on salt-restricted diets die SOONER. And Eskimos eat huge amounts of fat with no apparent ill-effects. And the average home-cooked roast dinner has LOTS of fat. Will we ban roast dinners?
6). The foods restricted are often no more calorific than those permitted -- such as milk and fruit-juice drinks.
7). Tendency to weight is mostly genetic and is therefore not readily susceptible to voluntary behaviour change.
8). And when are we going to ban cheese? Cheese is a concentrated calorie bomb and has lots of that wicked animal fat in it too. Wouldn't we all be better off without it? And what about butter and margarine? They are just about pure fat. Surely they should be treated as contraband in kids' lunchboxes! [/sarcasm].
9). And how odd it is that we never hear of the huge American study which showed that women who eat lots of veggies have an INCREASED risk of stomach cancer? So the official recommendation to eat five lots of veggies every day might just be creating lots of cancer for the future! It's as plausible (i.e. not very) as all the other dietary "wisdom" we read about fat etc.
10). And will "this generation of Western children be the first in history to lead shorter lives than their parents did"? This is another anti-fat scare that emanates from a much-cited editorial in a prominent medical journal that said so. Yet this editorial offered no statistical basis for its opinion -- an opinion that flies directly in the face of the available evidence.
Even statistical correlations far stronger than anything found in medical research may disappear if more data is used. A remarkable example from Sociology:"The modern literature on hate crimes began with a remarkable 1933 book by Arthur Raper titled The Tragedy of Lynching. Raper assembled data on the number of lynchings each year in the South and on the price of an acre's yield of cotton. He calculated the correlation coefficient between the two series at -0.532. In other words, when the economy was doing well, the number of lynchings was lower.... In 2001, Donald Green, Laurence McFalls, and Jennifer Smith published a paper that demolished the alleged connection between economic conditions and lynchings in Raper's data. Raper had the misfortune of stopping his analysis in 1929. After the Great Depression hit, the price of cotton plummeted and economic conditions deteriorated, yet lynchings continued to fall. The correlation disappeared altogether when more years of data were added."So we must be sure to base our conclusions on ALL the data. But in medical research, data selectivity and the "overlooking" of discordant research findings is epidemic.
"What we should be doing is monitoring children from birth so we can detect any deviations from the norm at an early stage and action can be taken". Who said that? Joe Stalin? Adolf Hitler? Orwell's "Big Brother"? The Spanish Inquisition? Generalissimo Francisco Franco Bahamonde? None of those. It was Dr Colin Waine, chairman of Britain's National Obesity Forum. What a fine fellow!
*********************
1 March, 2008
COCA COLA AND KIDNEY PROBLEMS

Another stupid "study" based on retrospective self-reports. I'll say no more. Such studies really are the lowest of the low and prove nothing. There must be a billion perople who are regular Coke drinkers. How come we don't have an epidemic of kidney problems? Kidney problems are in fact relatively rare. Popular summary below followed by journal abstract
It is well known that too much soda can increase the risk of diabetes and obesity. But when it comes to kidney problems, is there a difference between colas and other kinds of soda? Colas contain high levels of phosphoric acid, which has been linked to kidney stones and other renal problems.
Much of this conclusion stems from anecdotal and circumstantial evidence. So last year, a team of scientists at the National Institutes of Health took a closer look. In a study published in the journal Epidemiology, the team compared the dietary habits of 465 people with chronic kidney disease and 467 healthy people. After controlling for various factors, the team found that drinking two or more colas a day - whether artificially sweetened or regular - was linked to a twofold risk of chronic kidney disease. But drinking two or more noncola carbonated drinks a day, they found, did not increase the risk.
The authors of the study say more research is needed, but their findings support the long-held notion that something about cola - the phosphoric acid, for example, or the ability of cola to pull calcium from bones - seems to increase the risk of kidney stones, renal failure and other conditions affecting the kidneys.
Source
Carbonated Beverages and Chronic Kidney Disease.
By Saldana, Tina M. et al.
Background: Carbonated beverage consumption has been linked with diabetes, hypertension, and kidney stones, all risk factors for chronic kidney disease. Cola beverages, in particular, contain phosphoric acid and have been associated with urinary changes that promote kidney stones.
Methods: We examined the relationship between carbonated beverages (including cola) and chronic kidney disease, using data from 465 patients with newly diagnosed chronic kidney disease and 467 community controls recruited in North Carolina between 1980 and 1982.
Results: Drinking 2 or more colas per day was associated with increased risk of chronic kidney disease (adjusted odds ratio = 2.3; 95% confidence interval = 1.4-3.7). Results were the same for regular colas (2.1; 1.3-3.4) and artificially sweetened colas (2.1; 0.7-2.5). Noncola carbonated beverages were not associated with chronic kidney disease (0.94; 0.4-2.2).
Conclusions: These preliminary results suggest that cola consumption may increase the risk of chronic kidney disease.
Epidemiology. 18(4):501-506, July 2007.
New drug to beat breast cancer
A DRUG which could prevent thousands of young women developing breast cancer has been created by scientists. If given regularly to those with a strong family history of the cancer, researchers say it could effectively "vaccinate" them against a disease they are almost certain to develop. The drug, which attacks tumours caused by genetic flaws, could spare those who have the rogue genes the trauma of having their breasts removed. Currently, a high proportion of women who are told they have inherited the rogue genes choose to have a mastectomy as a preventative measure. Researchers hope such a vaccine will be available within a decade.
Flawed BRCA genes, which are passed from mother to daughter, are responsible for five to 10 per cent of breast cancer cases each year in Australia. Women with the rogue genes have an 85 per cent chance of developing the disease - eight times that of the average woman. Initial tests suggest that the drug, known only as AGO14699, could also be free of the side-effects associated with other cancer treatments, including pain, nausea and hair loss.
The drug, which is being tested on patients in the UK, works by exploiting the "Achilles heel" of hereditary forms of breast cancer, which is its limited ability to repair damage to its DNA. Normal cells have two ways of fixing themselves, allowing them to grow and replicate, but cells in BRCA tumours have only one. The drug, which is part of the class of anti-cancer medicines called PARP inhibitors, blocks this mechanism and stops the tumour cells from multiplying.
The researchers say the drug could also be used against other forms of cancer, including prostate and pancreatic, although further tests are needed. Researcher Dr Ruth Plummer, senior lecturer in medical oncology at Britain's Newcastle University, said: "The implications for women and their families are huge because if you have the gene, there is a 50 per cent risk you will pass it on to your children."
Source
****************
Just some problems with the "Obesity" war:
1). It tries to impose behavior change on everybody -- when most of those targeted are not obese and hence have no reason to change their behaviour. It is a form of punishing the innocent and the guilty alike. (It is also typical of Leftist thinking: Scorning the individual and capable of dealing with large groups only).
2). The longevity research all leads to the conclusion that it is people of MIDDLING weight who live longest -- not slim people. So the "epidemic" of obesity is in fact largely an "epidemic" of living longer.
3). It is total calorie intake that makes you fat -- not where you get your calories. Policies that attack only the source of the calories (e.g. "junk food") without addressing total calorie intake are hence pissing into the wind. People involuntarily deprived of their preferred calorie intake from one source are highly likely to seek and find their calories elsewhere.
4). So-called junk food is perfectly nutritious. A big Mac meal comprises meat, bread, salad and potatoes -- which is a mainstream Western diet. If that is bad then we are all in big trouble.
5). Food warriors demonize salt and fat. But we need a daily salt intake to counter salt-loss through perspiration and the research shows that people on salt-restricted diets die SOONER. And Eskimos eat huge amounts of fat with no apparent ill-effects. And the average home-cooked roast dinner has LOTS of fat. Will we ban roast dinners?
6). The foods restricted are often no more calorific than those permitted -- such as milk and fruit-juice drinks.
7). Tendency to weight is mostly genetic and is therefore not readily susceptible to voluntary behaviour change.
8). And when are we going to ban cheese? Cheese is a concentrated calorie bomb and has lots of that wicked animal fat in it too. Wouldn't we all be better off without it? And what about butter and margarine? They are just about pure fat. Surely they should be treated as contraband in kids' lunchboxes! [/sarcasm].
9). And how odd it is that we never hear of the huge American study which showed that women who eat lots of veggies have an INCREASED risk of stomach cancer? So the official recommendation to eat five lots of veggies every day might just be creating lots of cancer for the future! It's as plausible (i.e. not very) as all the other dietary "wisdom" we read about fat etc.
10). And will "this generation of Western children be the first in history to lead shorter lives than their parents did"? This is another anti-fat scare that emanates from a much-cited editorial in a prominent medical journal that said so. Yet this editorial offered no statistical basis for its opinion -- an opinion that flies directly in the face of the available evidence.
Even statistical correlations far stronger than anything found in medical research may disappear if more data is used. A remarkable example from Sociology:"The modern literature on hate crimes began with a remarkable 1933 book by Arthur Raper titled The Tragedy of Lynching. Raper assembled data on the number of lynchings each year in the South and on the price of an acre's yield of cotton. He calculated the correlation coefficient between the two series at -0.532. In other words, when the economy was doing well, the number of lynchings was lower.... In 2001, Donald Green, Laurence McFalls, and Jennifer Smith published a paper that demolished the alleged connection between economic conditions and lynchings in Raper's data. Raper had the misfortune of stopping his analysis in 1929. After the Great Depression hit, the price of cotton plummeted and economic conditions deteriorated, yet lynchings continued to fall. The correlation disappeared altogether when more years of data were added."So we must be sure to base our conclusions on ALL the data. But in medical research, data selectivity and the "overlooking" of discordant research findings is epidemic.
"What we should be doing is monitoring children from birth so we can detect any deviations from the norm at an early stage and action can be taken". Who said that? Joe Stalin? Adolf Hitler? Orwell's "Big Brother"? The Spanish Inquisition? Generalissimo Francisco Franco Bahamonde? None of those. It was Dr Colin Waine, chairman of Britain's National Obesity Forum. What a fine fellow!
*********************
