This document is part of an archive of postings by John Ray on Dissecting Leftism, a blog hosted by Blogspot who are in turn owned by Google. The index to the archive is available here or here. Indexes to my other blogs can be located here or here. Archives do accompany my original postings but, given the animus towards conservative writing on Google and other internet institutions, their permanence is uncertain. These alternative archives help ensure a more permanent record of what I have written.
This is a backup copy of the original blog

Below is the backup of this blog for March, 2024. To access the backups in earlier years, click here
27 March, 2024
Four Years Later
Has the dust settled?
Far from it. It is everywhere. We are choking on it. The storm cloud comes in many forms: inflation, learning losses, ill-health, high crime, non-functioning government services, broken supply chains, shoddy work, displaced workers, substance abuse, mass loneliness, discredited authority, a growing real estate crisis, censored technology and overweening state power.
For that matter, consider that Easter, the day to celebrate the Son of Godĺs triumph of life over death, itself was cancelled for public worship just four years ago. That actually happened. Not even at the height of World War II was there a consideration of such a thing, or even cancelling baseball. When the idea was suggested in a famous movie script, Spencer Tracy asked ôWhy would you abolish the thing you are trying to preserve?ö (Woman of the Year 1942).
Good question. What precisely was the point of the hell we went through? Who did it and why? Why did it last so long? Why has there been no official accounting?
The lack of any real accountability or even so much as an apology is a foreshadowing: they will keep their newfound powers and try it all again.
Meanwhile, the world is on fire with war, mass killings, crime, hunger and revolution.
All of this traces to lockdowns that began March 2020, the subject about which no one in polite society speaks. It was a painful period, to be sure. The people who did this to us are hoping that we are too traumatised to pursue accountability, much less justice. To the extent we feel that way, we are playing right into their hands.
Even now, there are hundreds and even thousands of questions.
Why were there no widespread seroprevalence tests of the population before locking down? This would have been a great way to measure the level of pre-existing exposure and assess whether Deborah Birxĺs stated objective to bring about Zero Covid had any chance of success.
Where did the World Health Organisation get the completely bogus 3.4% infection fatality rate number and why did it push it out?
For that matter, why did the lockdown architects not bother with the vast literature already extant, accepted as definitive in the public-health world, that lockdowns achieve only destruction and there was no form of physical intervention that had any hope of stopping a virus destined to spread to the whole population?
These were known about at the time, as were the broad outlines of the impact of this virus. So let there be no more talk about how little we knew at the time. We knew.
We still donĺt know:
how they talked Trump into reversing his anti-lockdown stance on or around March 10th 2020;
to what extent the sudden spread of the virus was fuelled by testing or even how accurate the tests were;
whether the sudden wave of early death was panic-based or iatrogenic or actually the virus;
how it is that previously obscure agencies gained the power to manage the U.S. workforce and censor media;
who precisely gave the order to lock down U.S. hospital care and why;
how it came to be that the Government tried to drive conventional antivirals out of the marketplace;
who had pre-written the thousand-page bills that authorised $2 trillion in spending that broke the budget and unleashed an experiment of universal basic income.
Strangely, much of this can be explained by the crazed ambition to preserve population-wide immunological na´vetÚ while waiting for the vaccine to arrive in mid-November, eight months later. Was that always the idea, in which case the ô15 Days to Flatten Curveö was known to be complete gibberish? If that is actually true, the arrogance and sadism of the policy goal here boggles the mind.
And if that is true, why? Was it to deploy a new platform technology called mRNA that otherwise would obtain no chance for a generalised trial through normal paths? Is that the reason that Anthony Fauci went after the J&J vaccine early on, as a tactic to drive it out of the market and prepare a clean slate for Pfizer and Moderna?
If that was the goal, was it ever stated in private and by whom? Who knew the goal from the beginning?
That anyone among the ruling class could even consider conscripting the whole population into such a biological experiment gives rise to wartime ghouls of a past we thought we had left behind.
These questions only scratch the surface. Even after four years of researching this topic as part of a very large team that has scoured through a million pages of documentation and stories, having written two books and many thousands of articles, and being fuelled by a burning desire to know, most of us still have no clear answer to the profound question: why and how did this happen to us?
There are many theories, all with plausibility but none with the capacity to explain the whole.
We might say that pharma was behind the whole thing. That seems credible. The goal of testing mRNA on the global population explains a lot, especially given the trumped-up emergency situation. But the very notion that hundreds of governments around the world became surreptitiously captured stretches plausibility.
We might observe that digital tech manipulated policy to give itself a boost. The first big and viral article on the whole lockdown idea was by Thomas ôHammer-and-Danceö Pueyo, a CEO of an online learning hub that became a huge winner. Streaming platforms benefited and so did Amazon as a grocery and goods source, as did Uber Eats and DoorDash and others such as Zoom.
But are we really supposed to believe that human liberties the world over were wrecked to boost profits of this one industry? Again, thatĺs a stretch. And the same could be said of the theory that media was the driving force. Yes, they won big time, deploying censorship as an industrial tactic against new media startups. But how in the world would they have gained so much power the world over?
Then there is the view that the whole monstrous scheme was concocted to drive Trump out of office by creating chaos and greenlighting mail-in ballots that are difficult if not impossible to check for validity. That seems to check many empirical boxes. No question that there was some major effort to confuse the public as if the presence of the virus was a metaphor for the Trump administration itself that needed to be strangled.
There is surely truth here but how does that account for the hundreds of other governments around the world following the same path? That the response was not just national but global raises real questions.
In that context we might draw attention to the role of the CCP, which first deployed lockdowns amidst theatrically produced videos of people dying in the streets and then leaning on its power over the World Health Organisation to recommend lockdowns to the whole planet.
Thereĺs truth in that theory too.
In the deeper realms, we are wise to visit the depths of the RFK Jr. book The Wuhan Cover-Up, which explains the history of the U.S. bioweapons programme dating back to the end of World War II. There are secret labs all over the world supported by the U.S., including in Wuhan. Their activities and funding are covered by classified restrictions from public access.
The purpose of gain-of-function research is said to be not to discover solutions to emerging new pathogens but to create new pathogens with antidotes that we have and the enemy does not have.
Was the release of this one pathogen part of this programme? If so, that would explain why the intelligence and security bureaucracies became involved very deeply early on and also explain why so many FOIA requests about every aspect of this come back heavily redacted and why we are having such a hard time getting information in general.
Any time a policy matter touches the realm of national security and intelligence, it is covered by an impenetrable veil of secrecy that no law or court seems to be able to control. This site has often explored this path of inquiry too with a great deal of evidence supporting it. In this case, we are really talking about a next-level theory, that of a digital-age coup by Deep State masters against civilian society and democracy itself.
You can probably generate another 10 or more compelling theories about the whole episode. Connecting the dots is a full-time job.
A wise man mentioned to me yesterday the astounding fact that we still do not have a full explanation of why and how the Great War came to be. That war ended old-world civilisation as we knew it. In some ways, now looking back, it was the beginning of the end of what we might call high civilisation and the prospects for peace. It unleashed the Bolshevik Revolution, caused Western-style freedoms to be mitigated by administrative state actors, introduced the idea of total war, recruited whole populations to become soldiers and otherwise shredded near-global expectations for ever rising prosperity and peace.
And yet, we still donĺt know fully why or how it happened. Error piled on error and malice on malice. Once that kind of sadistic chaos tempts a ruling class, many other institutions sign up to join the party of pillage and plunder and society finds itself picked apart by interest groups that care nothing for the good of all, much less human rights.
Thatĺs a pretty solid description of what happened to us four years ago. They broke the world.
[The Great War was certainly a great horror and a great turning point. It seems crazy in retrospect. I have argued, however, that it was a rational response to the circumstances of its time:
http://jonjayray.com/short/ww1.html
JR]We may never get the truth but we can get closer to the truth. There will be no stopping the efforts.
https://dailysceptic.org/2024/03/25/four-years-later/
*************************************************27 March, 2024
Lockdowns could cause more harm than Covid-19 and there was no evidence that wearing masks was useful
Germany's top public health agency knew that Covid lockdowns could be more damaging than the virus itself as early as December 2020 and said mask mandates were not backed by evidence, it has been revealed.
Newly published documents from the Robert Koch Institute (RKI) show its researchers explicitly warned that their analysis showed lockdowns in Africa showed 'an expected rise in child mortality'.
'The consequences of the lockdowns are in parts more severe than the virus itself,' the December 2020 report said, with another document dated to October 2020 suggesting that there was 'no evidence' to support that FFP2 medical masks could prevent the spread of Covid.
But the findings were never made public, despite researchers clearly advocating for the open communication of their research in meeting minutes, with the German government choosing to pursue legislation their own researchers advised against.
The revelations come after a two-year legal battle between the RKI and German magazine Multipolar, which ultimately won the court case to publish documents that were heavily redacted by the health agency.
Multipolar has since launched another legal claim in an attempt to secure full access to the unredacted documents, which may conceal a trove of Covid policy recommendations that the RKI and the German government opted not to share with the public.
The saga now threatens to trigger a fallout in the German government, with Bundestag Vice President Wolfgang Kubicki telling German media: 'The protocols of the RKI crisis team, some of which have now been released, raise considerable doubts as to whether the political measures to deal with the corona pandemic were really taken on a scientific basis.'
Kubicki told German outlet Bild that 'the top of the RKI, of all people, followed the political guidelines of the respective federal government and thus provided the necessary scientific facade for Corona policy.'
Seven in ten scientists say ministers failed to consider the long-term damage of lockdowns during the Covid pandemic
He also called on Germany's Federal Minister of Health, Karl Lauterbach, to 'present all protocols to the public without redactions in order to create complete transparency about the internal discussions and the basis for decisions.
'If Karl Lauterbach does not follow my request, as a parliamentarian I will work to persuade him to make this disclosure so that the clarification can finally be satisfied.'
Meanwhile, the former leader of Germany's Christian Democratic Union party Armin Laschet has declared the RKI must go public with its findings.
Speaking with German broadcaster ZDF, the parliamentarian said: 'We have to disclose everything.
'You can see how differentiated the discussions were at the RKI back then and how little of this diversity of opinion ultimately found its way into concrete policy,' he continued, recalling how debates over Covid policy became 'moralised'.
'Either you are for one measure or you are a Corona denier. But there was a lot in between,' he concluded.
Meanwhile, a minute from an RKI meeting in January 2021 expressed concerns with the viability of the AstraZeneca Covid vaccine, with researchers warning its use 'should be discussed' because the jab was 'not as perfect'.
That same jab - that was offered to millions in the UK - was later discontinued and not offered as a booster after reports surfaced of people developing blood clots in combination with low platelet levels.
The shocking revelations come as public health experts in the UK slammed the government's Covid inquiry for 'bias', claiming it has failed to investigate the harmful impact of lockdown on British society.
More than 50 scholars and academics from some of the UK's top universities wrote to inquiry chairman Baroness Heather Hallett earlier this month urging her to 'address its apparent biases, assumptions and impartiality'.
They accuse the inquiry of 'not living up to its mission to evaluate the mistakes made during the pandemic', including whether measures such as lockdowns and restrictions on mass gatherings were 'appropriate'.
Letter co-author Dr Kevin Bardosh, director of think-tank Collateral Global, accused the inquiry of handing 'softball' questions to architects of government policy, while 'grilling' witnesses who were opposed to mass restrictions on public freedoms.
He told the Mail: 'The inquiry is not seriously questioning their (scientific advisers') assessments around the justification for their policies.
'The inquiry is not interested in whether these policy decisions were good for the country, and that seems a mistake.'
The terms of reference setting out the scope of the inquiry were established by the Government following public pressure for an inquiry.
But Dr Bardosh accused Hugo Keith KC, lead counsel to the inquiry, of being more 'obsessed with reading out swear words in private WhatsApp messages than getting to the substance' of decision-making.
He said: 'He seems to be concerned a lot with political theatre and having these 'gotcha' moments.'
Cancer specialist Professor Karol Sikora, who signed the letter, described the inquiry as 'completely useless'.
He added: 'It is structured to assess blame and not the scientific basis of the decision making. That's the difference between lawyers and scientists.
'The decisions made during the pandemic were clearly wrong - 'how' wrong has to be a scientific assessment.
'The current framework for the current inquiry is a legal one - totally unsuited to addressing the key questions.
'We're not interested in WhatsApp gossip. We have to learn from the past - it's not about the apportioning of blame but simply how to do better next time.'
The inquiry began hearing evidence in June last year, with testimony from the likes of prime minister Rishi Sunak, Covid-era premier Boris Johnson, and ex-health secretary Matt Hancock, as well as a host of the most senior scientific and medical advisers to the Government.
The bill for the inquiry has already topped £78 million up to the end of last year, according to its latest financial report.
In its letter, the group said: 'The inquiry originated in legal petitions brought by bereaved family groups. Yet there has been little opportunity for petitions to be brought by those who have suffered from the negative effects of pandemic policy decisions.
'This is preventing a more holistic assessment of impacts on population health and wellbeing. This lack of neutrality appears to have led to biassed reasoning and predetermined conclusions, for example, to lockdown faster next time.'
It said the inquiry, which is due to run until 2026, has 'adopted a legal format that prevents a systematic evaluation of the evidence by biomedical and social scientists on the harms of restrictions to the British public' and is instead 'focused on who did or said what, rather than asking fundamental scientific questions'.
It said the probe 'appears unsuited to the task' of investigating 'the interplay between harms, benefits and best practice' in order to prepare for the next pandemic.
*************************************************
"COVID Revisited" Conference to Shed Light on Australia's Pandemic Response
Almost four years since the pandemic began, COVID-19 continues to leave its mark on Australia, affecting healthcare and society in general. While the vaccines offered some degree of protection, controversies remain around the pandemic response. These include a case brought against pharmaceutical giants Pfizer and Moderna and calls seeking transparency from the Australian government about its pandemic measures. TrialSite has reported before on Australian analysts challenging the pandemic narrative driven by the government.
To discuss the lessons learned and examine past challenges, the Australian Medical Professionals’ Society (AMPS) is organizing a conference named “COVID Revisited: Lessons Learned, Challenges Faced, and the Road Ahead.” The event aims to provide a platform from which to discuss the government’s decisions during the pandemic and policies to guide future responses.
As time passes, the controversies surrounding the lockdown measures and vaccine mandates in Australia seem to intensify. TrialSite previously reported on a legal case filed against Pfizer and Moderna in the Federal Court of Australia accusing them of lacking transparency regarding alleged DNA contaminants and GMOs in their vaccines. This case was filed by Dr. Julian Fidge and handled by lawyer Katie Ashby-Koppens and former barrister Julian Gillespie.
Providing an update in a February 2024 Substack article, Gillespie explained that the presiding judge, Hon Helen Mary Joan Rofe, had at the time delayed a final decision on the defendant's application for a case dismissal. However, on March 1, 2024, Rofe dismissed Fidge’s lawsuit against Pfizer and Moderna. For the time being, this ruling has put a halt to any likely legal challenges gaining traction against the mRNA vaccines.
We also reported in February 2024 that Australians were demanding a COVID-19 Royal Commission to investigate the vaccine mandates and pandemic measures implemented in the country. Ashby-Koppens was among those calling for this Royal Commission. According to Gillespie, the Senate Terms of Reference Committee is currently deliberating this.
Despite Rofe’s ruling, the critics are not backing down. With the AMPS’s conference looking to help people learn and discuss better ways to handle future pandemics through the “COVID Revisited” program and the ongoing process at the Senate Terms of Reference committee, the critics believe that the upcoming conference “reflects the Australian people's wish for a review of the government response to COVID-19.”
The “COVID Revisited” conference
The conference is scheduled for April 2, 2024, and will take place in the State Library NSW Auditorium. According to AMPS, top medical and academic professionals from around the world will be in attendance, with the event garnering support from notable organizations like the National Institute of Integrative Medicine (NIIM), Australasian College of Nutritional and Environmental Medicine (ACNEM), World of Wellness International (WOW) and Children’s Health Defense Australia Chapter (CHD).
Speaking about the conference’s mission, AMPS secretary Kara Thomas stated, "Our mission is clear. We aim to generate tangible policy recommendations that substantially influence the management of future pandemic crisis situations."
Emeritus Professor Robert Clancy, one of the speakers, provided insights into the event’s structure and its focus on examining the government's handling of the COVID-19 response. “This symposium is structured to reflect the collective views of those involved in this response,” Clancy said, “with a particular focus on lessons learned as to mistakes made and how best to go forward with the best plan to handle health challenges of similar ill when next encountered.”
He further stated, “Presentations from professionals covering these disciplines will be followed by an interactive workshop with an expert panel charged with identifying outcomes. The day will conclude with a reception allowing informal discussion amongst participants and attendees. A book including presentations and outcomes will be published.”
According to AMPS, the conference will produce a set of well-defined resolutions, to be shared widely with practitioners, public health authorities and government bodies. These resolutions will identify practical measures to ensure safe and effective responses. In doing so, they aim to reduce mishandling in crisis management that could potentially compromise Australians’ health.
Progress achieved and challenges faced during the pandemic
The Australian government’s pandemic measures yielded a mixed set of outcomes. The Financial Times reported that while Australia’s initial zero-COVID strategy showed positive results in containing the virus, some critics argued that it was too strict with potential adverse economic implications.
The government’s actions included closing international borders to non-residents and, at times, restricting internal state border crossings. Widespread testing and contact tracing enabled authorities to suppress community transmission and by June 2021, Australia had recorded low COVID-19 case numbers compared to other countries.
However, these actions by the government had some negative impact on businesses and families, as business owners complained that the lockdown lingered for too long. According to a Lancet study, the Australian government was accused of discriminatory travel restrictions against specific countries, leaving many Australians stranded abroad for long periods. Moreover, as new variants emerged, maintaining zero-COVID became increasingly difficult. The Australian authorities then shifted their focus to pushing vaccination campaigns and moved from their zero-COVID policy in September 2021.
*************************************************
26 March, 2024
Pfizer Finally Releases Myocarditis Study for Children Who Received COVID-19 Vaccine
Pfizer and its partner BioNTech have finally released the results of clinical trials exploring whether their COVID-19 vaccine causes subclinical heart inflammation. The companies found that multiple vaccine recipients suffered heart-related symptoms, but said none met the definition of myocarditis, or heart inflammation.
Researchers with the companies and other institutions analyzed the levels of troponin I, a sign of possible heart damage, in children aged 5 to 30 before and after receipt of the Pfizer-BioNTech vaccine. They also monitored participants for heart-related symptoms, including chest pain. If patients suffered symptoms, doctors examined them and researchers performed other tests, such as an electrocardiogram, as well as additional troponin measurements.
Ten vaccinated participants, including six under the age of 12, reported relevant symptoms. The researchers, though, said none had myocarditis after additional testing.
Among the younger children, half of the participants with the symptoms underwent troponin evaluations and four had electrocardiograms. All the results were normal, according to the researchers. One of the six had a cardiac MRI performed, and the MRI came back with abnormal results. But the results suggested viral infection, not cardiac abnormalities, they said.
Among the four people in the older group who experienced symptoms, one suffered chest discomfort and trouble breathing on the same day as receiving the shot. An electrocardiogram the next day revealed an ST elevation, and troponin levels in the individual were also significantly elevated.
But an echocardiogram and cardiac MRI both returned normal, and researchers said the case did not constitute myocarditis or a related condition called pericarditis.
ôI donĺt know what to make of that,ö Dr. Andrew Bostom, a heart expert who was not involved in the study, told The Epoch Times after reviewing the paper. ôThat could have been clinically defined as some sort of abnormality, some sort of cardiac abnormality.ö
The other cases among the older group were also ruled not to be myocarditis, although the troponin data for three of the four was ônot reported,ö the researchers said.
That missing data is concerning, Dr. Bostom said.
Elevated Troponin
In total, researchers found 20 of about 2,000 vaccinated participants had elevated troponin levels.
The researchers compared the percentage of participants who had elevated troponin to other groups. For 12- to 30-year-olds, the control group was composed of healthy people who had previously received two or three doses of the vaccine. That group received a placebo, while the study group received another shot.
For 5- to 11-year-olds, the control group was comprised of unvaccinated children who received placebos while the study group received one to three doses of the Pfizer-BioNTech vaccine.
Across both trials, exclusions included people with a history of severe adverse reactions to vaccines, and no participants had prior myocarditis.
A lower percentage of 12- to 30-year-olds who received a new vaccine dose had elevated troponin shortly after vaccination, when compared to the control group. The testing was done on the fourth day after receipt of a vaccine dose or placebo.
But one month after a dose or placebo, the percentage was higher among the newly vaccinated arm.
The rate of COVID-19 was also higher among the newly vaccinated people in the older group, with eight cases compared to two in the control arm.
In the younger children, the elevated troponins were higher among the vaccinated after each dose. No elevated troponin cases were detected in the unvaccinated cohort.
The trials reported in the paper were aimed at assessing the risk of subclinical myocarditis, or heart inflammation without symptoms. The U.S. Food and Drug Administration required them when approving the Pfizer-BioNTech shot in 2021, after myocarditis became known as a side effect of the Pfizer and Moderna vaccines, which both utilize messenger RNA (mRNA) technology.
The larger trial, which covered 12- to 30-year-olds, was supposed to be done in mid-2022, with results submitted to the administration by the end of that year. But the deadline was pushed back at Pfizerĺs request. The other trial had been scheduled to be completed on Nov. 30, 2023.
The new paper was submitted to the journal on Nov. 13, 2023, the journal said.
A previous study found elevated levels of troponin among people who received Modernaĺs shot, raising concerns of subclinical myocarditis.
Measurements?
The new paper did not provide evidence that Pfizer-BioNTech vaccination causes elevations in troponin, so thereĺs no point in measuring troponin levels in asymptomatic vaccine recipients, the authors said.
Dr. Bostom agreed.
ôBut thatĺs not exactly an earth shattering finding,ö he said. ôThatĺs the way youĺre supposed to use troponin. Weĺre not supposed to go around and screen everyone for troponin elevation.ö
Measuring troponin after symptoms like chest pain appear is useful, he added later.
Dr. Peter McCullough, a cardiologist who also reviewed the study, said that he found it lacking.
ôFull comparisons of mean, median, range, stratified by cumulative doses received with parametric statistics would be needed in a thorough cardiac toxicology study,ö Dr. McCullough told The Epoch Times in an email.
ôSelection bias, loss to followup, and the majority of authors having a vested financial stake in the Pfizer/BioNTech COVID-19 vaccine are additional concerns. With the mass of studies demonstrating mRNA COVID-19 vaccination causes serious and fatal myocarditis, this study is not reassuring to the cardiovascular community,ö he added.
Listed limitations in the new paper included being underpowered to detect myocarditis cases, while the lengthy conflicts of interest section included notes on many authors either being current or former Pfizer employees. The paper was also funded by Pfizer and BioNTech.
***********************************************
Little Known about mRNA and Spike Protein Biodistribution Three Years into Mass Vaccination Campaign
Alarming Conclusions from Russian Analysis of Studies
By Peter A. McCullough, MD, MPH
I remember when the mRNA COVID-19 vaccines rolled out in December, 2020. I asked some of the doctors a few questions about the novel products. Where do they go in the body? How long do they last? No one knew the answers yet throngs came forward and took the jab.
Now a Russian analysis of the biodistribution data on lipid nanoparticles laced with mRNA has been published by Pateev et al. The conclusions are shocking especially considering we are three years into a global mass vaccination campaign with shots every six months.
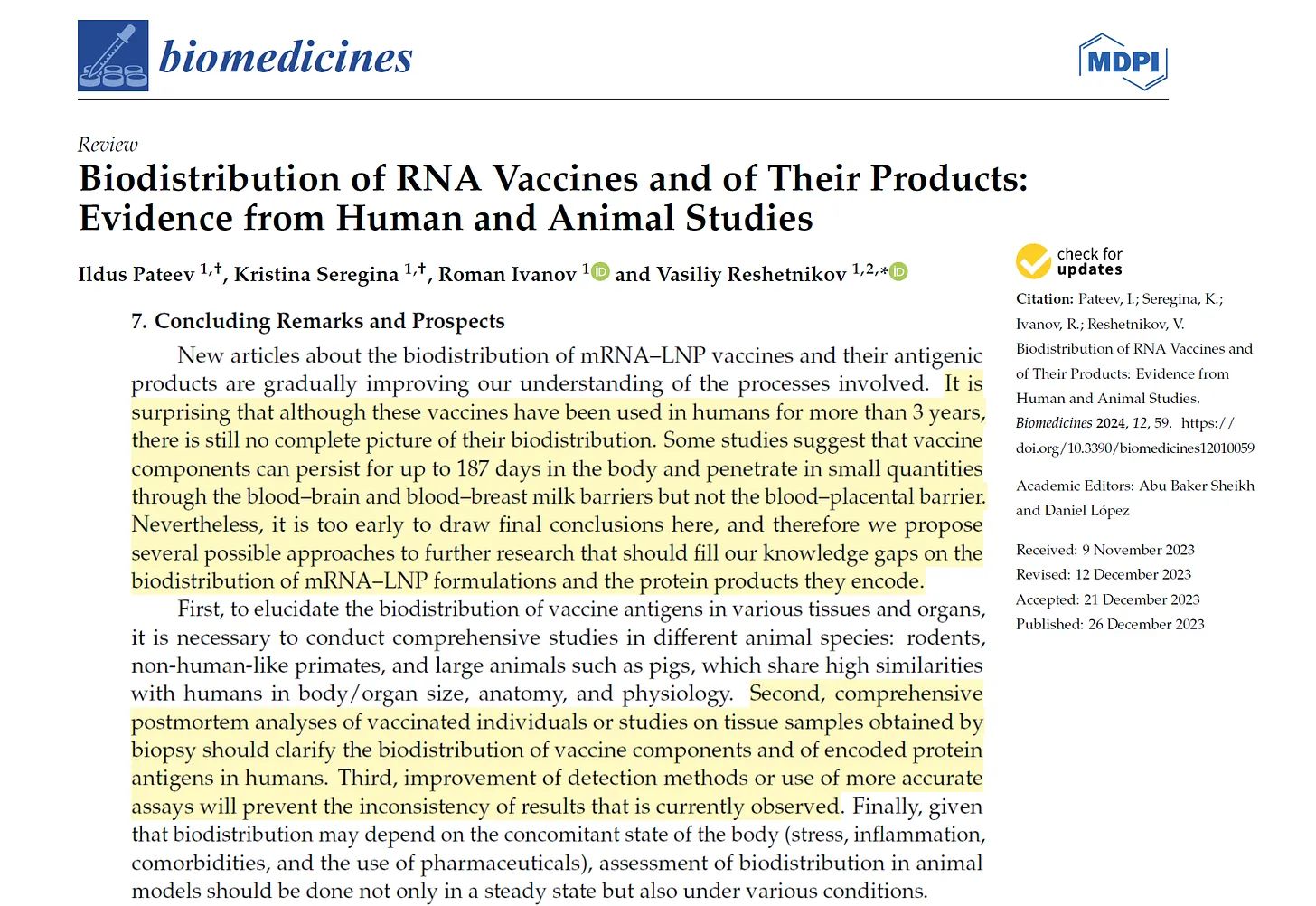
This image from the manuscript is not reassuring for a vaccine, which one would anticipate should remain in the deltoid muscle, incite local antigenic stimulation, and then have the lymphatic and immune system produce clearance of the foreign material and confer durable immunity. As you can see, mRNA vaccines do nothing of the sort. The widespread distribution, long duration of action, and dangerous unending production of the damaging and potentially lethal Spike protein continue to cause great alarm among doctors, scientists, and the public who are asking questions regarding the biological fate of these new products
*************************************************
25 March, 2024
The Harm of College Vaccine Mandates
Who would have believed weĺd still be talking about Covid vaccine mandates in 2024, but given how resistant authority figures are to accepting reality, or defeat or acknowledging mistakes, it seems likely weĺll unfortunately be subjected to talking about them forever.
Dozens of colleges are continuing to enforce vaccine and booster mandates on students, refusing to accept, in the face of all available evidence and data, that there is no external health benefit whatsoever to forcing 18-year-olds to get injected with a vaccine with minimal, transient benefits but with potentially harmful side-effects.
This is made even more frustrating by the fact that the former director of the FDA recently admitted that the Covid vaccine approvals process, which gave colleges and universities licence to unnecessarily force mandates onto young people, was catastrophically and fatally flawed.
Now a few researchers have turned their efforts towards attaching specific, conclusive data to expose just how damaging and harmful these mandates have been for young college students.
And itĺs not good news.
Covid Booster Mandates Were Completely Unnecessary
The results from this study in the Journal of Medical Ethics are jaw-dropping, both for the harms caused by booster mandates and how utterly meaningless those mandates are to preventing any negative outcomes from Covid.
As the authors explain, thousands if not millions of college students risked having their lives and educations upended if they refused to comply with Covid booster mandates. One would imagine that to risk the possible futures of their students, colleges and universities must have required clear-cut evidence that such mandates were necessary, effective and justifiable given the epidemiological circumstances.
That evidence did not exist.
The underlying assumption of booster mandates is that a mass wave of hospitalisations and serious Covid-caused health issues would occur if students werenĺt forced to stay Ĺup to dateĺ with their vaccinations. Another assumption was that immunity from previous infection was effectively nonexistent.
As this study clearly shows, both assumptions were wildly, unimaginably wrong.
Based on an examination of booster efficacy, specifically among the 18-29 age group that makes up the overwhelming majority of college and university students, the authors estimated that 22,000-30,000 young adults must be boosted to prevent one COVID-19 associated hospitalisation.
And even thatĺs an overstatement. Itĺs 22,000-30,000 uninfected adults.
We estimate that 22,000-30,000 previously uninfected adults aged 18-29 must be boosted with an mRNA vaccine to prevent one [COVID]-19 hospitalisation.
Given the prevalence of infection-acquired immunity, especially among young people, by the time booster mandates came into effect in late 2021 and early 2022, itĺs likely that schools with large enrollments in the 20,000-25,000 range may not have prevented a single Covid hospitalisation with booster mandates.
Not one.
Assuming 70% of students had already contracted Covid by 2022 ľ an easily achievable number considering seroprevalence estimates at that time ľ a school with 20,000 students would also have had 14,000 with natural immunity. Meaning that at the higher end of the studyĺs estimates, youĺd have to look through five major universities with booster mandates before finding a single avoided Covid hospitalisation.
This potentially life-changing policy, affecting millions of students and their futures, was almost entirely meaningless. And thatĺs only telling half the story.
ĹNet Expected Harmĺ
Beyond the clear uselessness in terms of reducing hospitalisations, the researchers also found that there was likely a ônet expected harmö from mandates thanks to the often-ignored vaccine side-effects.
Using CDC and sponsor-reported adverse event data, we find that booster mandates may cause a net expected harm: per [COVID]-19 hospitalisation prevented in previously uninfected young adults, we anticipate 18 to 98 serious adverse events, including 1.7 to 3.0 booster-associated myocarditis cases in males, and 1,373 to 3,234 cases of grade 3 or higher reactogenicity which interferes with daily activities.
Effectively, for every 22,000-30,000 students subjected to booster mandates, there could be as many as nearly 100 serious adverse events. And one prevented hospitalisation.
Not to mention quite literally thousands of side-effects that could interfere with ôdaily activitiesö.
So in order to possibly prevent one hospitalisation among tens of thousands of students, colleges and universities essentially subjected young adults, especially men, to a risk of serious adverse effects that was 18 times to 98 times higher.
A graphic from the study indicates how significant the gap between benefits and harms is in practice.
If youĺre wondering how that makes any sense, I can assure you that it doesnĺt. And again, these risk-benefit ratios fail to factor in the prevalence of natural immunity among young people. As the researchers point out, this obvious but purposefully ignored reality makes this policy even more inexcusable.
ôGiven the high prevalence of post-infection immunity, this risk-benefit profile is even less favourable,ö the authors write. That makes the entire policy ôunethicalö, meaning that those impacted by it are more likely to be harmed by the intervention than helped.
University booster mandates are unethical because: 1) no formal risk-benefit assessment exists for this age group; 2) vaccine mandates may result in a net expected harm to individual young people; 3) mandates are not proportionate: expected harms are not outweighed by public health benefits given the modest and transient effectiveness of vaccines against transmission; 4) U.S. mandates violate the reciprocity principle because rare serious vaccine-related harms will not be reliably compensated due to gaps in current vaccine injury schemes; and 5) mandates create wider social harms.
Quite literally, there is a ônet expected harmö for individual young people that were coerced into getting boosted rather than see their educational careers destroyed or futures derailed.
The very ôexpertsö and administrators who admonished critics with endless appeals to authority, claiming that they were ôfollowing the scienceö while detractors were ôanti-scienceö extremists, likely caused a net harm to thousands, if not millions of their students.
Booster mandates were unnecessary, unethical and harmful, with vanishingly small benefits and massive increases in risk. Many schools have quietly dropped their policies and mandates without acknowledging the harm they caused. But that doesnĺt make it any less real, or any less inexcusable.
The actual science said they were wrong. Yet as has been so often the case during Covid policy debates, the actual science took a back seat to panic, fear, malicious coercion and inexcusable ignorance.
https://dailysceptic.org/2024/03/23/the-harm-of-college-vaccine-mandates/
***************************************************Vaccine mandates for NSW health workers to be dropped
NSW health workers will no longer need to be vaccinated against COVID-19 under a plan to phase out vaccine mandates.
Health workers in NSW will no longer be required to be vaccinated against COVID-19 as the state government moves to ditch mandates for the sector.
Health Minister Ryan Park confirmed the change would be going ahead after consulting with the state's health workforce.
'We know that COVID is still around but we've got to get back on with life,' he told Sydney radio 2GB.
'That means having a look at the measures we put in place during this period and seeing whether they still apply.
'We think this is one that we can engage with the workforce on and have a look to see if it's still applicable now.'
Public health orders mandating vaccines for health professionals were brought in during the pandemic and workers who refused either quit or were sacked.
While the order expired in November 2022, some workplaces have still been able to require mandatory vaccination under their own work, health and safety obligations.
Mr Park said if a decision was made to drop the mandates, workers who lost their jobs would be able to reapply to available positions through the usual recruitment processes.
He said COVID was still a public health threat and encouraged people to keep up with their vaccinations.
'But we've also got to make sure that we get on with running a health system after COVID and we can't continue in the same way that we did in the middle of the pandemic,' he said.
https://www.dailymail.co.uk/news/article-13233833/Vaccine-mandates-NSW-health-workers-dropped.html
*************************************************24 March, 2024
More Gobbledegook about masks
Smile Free has often highlighted the utter nonsense espoused by the U.K. Governmentĺs public health experts and plethora of advisers on the issue of community masking. Who can forget the flip-flops of Dr. Jenny Harries and Professors Whitty and Van-Tam in June 2020, transitioning from urging healthy people not to wear face coverings into strident pro-mask advocates? Or the absurd claim of Professor Trish Greenhalgh that science is the ôenemy of good policyô? But, not to be outdone, the Scottish leg of the U.K. COVID-19 Inquiry has confirmed that the gobbledegook around masks was not confined to England but also infected the Ĺexpertsĺ operating north of the border.
After the extended ramblings of Nicola Sturgeon ľ trying, in vain, to justify the convenient deletion of all her Covid-related WhatsApp messages ľ we were treated to the appearances of Professor Jason Leitch (National Clinical Director), Humza Yousaf (Scotlandĺs First Minister), Colin Poolman (Royal College of Nursing Scotland Director) and Devi Sridhar (Professor of Global Public Health). Chunks of their testimonies constitute a mix of ignorance, a detachment from reality and Monty Pythonesque comedy.
Did anyone understand the mask rules?
Clearly, Humza Yousaf (the then Scottish Health Secretary, no less) didnĺt. During Leitchĺs appearance at the inquiry it was revealed that, in November 2021, Yousaf asked Leitch whether he needed to wear a mask when stood talking at a social event. Leitch responded:
Officially yes. But literally no one does. Have a drink in your hands at all times. Then youĺre exempt. So if someone comes over and you stand, lift your drinků Thatĺs fun. Youĺll go down a treat.
When challenged by the Lead Counsel as to whether this was an example of a ôwork-aroundö to ôget out of complying with the rulesö, Leitchĺs denial was less than concise:
There was an ambiguity here that I faced as well, as we re-opened in this period, of the country, and that ambiguity was that we were allowing social occasionsů And there was an ambiguity around mask-wearing when you were seated, eating, drinking, because these events are ľ often involve a dinner. And there was some difficulty with the interpretation of mask-wearing inside those rooms when you were eating, drinking or moving aroundů but there were occasions, particularly when the country was opening up again, where there was of course nuance around the guidance and the rules, and this I think was one of those occasions: when you were at a dinner, eating and drinking, and somebody approached youů I think this was a tricky area that I found tricky as well.
Well, that clears things up!
And ľ as observed by the KC during his questioning of Yousaf ľ ôWhen you, the Cabinet Secretary for Health and Social Care, feel the need to clarify the rules about face masks, what chance do others have in understanding the rules?ö When this absurdity was put to Leitch, the Clinical Directorĺs response was, inadvertently, illustrative of the mask nonsense:
I understood the rules and I understood what we were trying to do, but the reality of life and the environment in which we were trying to do these things perhaps suggests this guidance was nuanced rather than entirely right.
If only our leaders had paid a smidgeon more attention to the ôreality of lifeö we wouldnĺt all have had to endure the imposition of masks (or, indeed, many of the other counterproductive Covid restrictions).
If only the masks had been a tad smaller
Colin Poolman, representing the Scottish RCN, lamented that the face masks provided were often too large for the NHS workforce. ôNursing is a predominantly female profession and many of the masks were not designed in smaller sizes so we had huge issues at times,ö he told the inquiry, implying that a better-fitting strip of plastic would have provided an effective shield against the SARS-CoV-2 pathogen. Given that the use of surgical masks to block respiratory viruses is akin to using a tennis net to hold back grains of sand, itĺs hard to see how a bit less of a gap around the edges would have made any significant difference to the level of protection afforded.
Neglect of inconvenient evidence
The wealth of pesky evidence demonstrating that face coverings constitute an ineffectual viral barrier has always been a problematic truth to the pro-mask brigade: their guiding rule seems to be, ôIf the science doesnĺt support our ideological preferences, dismiss it.ö In Scotland, the doppelganger to Englandĺs Trish Greenhalgh, appears to be Professor Devi Sridhar.
Sridhar is saturated with globalist credentials. She is Professor of Global Public Health at Edinburgh University and has worked closely with the United Nations, the World Health Organisation, the Wellcome Trust and the World Bank. During her testimony at the COVID-19 Inquiry, Sridhar demonstrated a conveniently flexible attitude to empirical research. For instance, while bemoaning that ôwe spent too long debating whether masks workö, Sridar asserts that ôin clinical settings they work, surgeons use them, on construction sites, the mask itself worksö. This esteemed academic seems blissfully unaware that surgeons primarily don face coverings to avoid potential exchange of bodily fluids (such as saliva and blood) rather than to reduce the transmission of viruses. And as for construction sites, keeping dust and fragments of concrete and masonry at bay is a somewhat different challenge to avoiding inhalation of microscopic pathogens.
Like many of her pro-mask public health colleagues, Sridhar appears to struggle to grasp what happens in the real world. Thus, she rightly acknowledges that ômasks at a population level are often not used correctly, people wear them over their mouth not their nose, they take them off to eat and drinkö, but then asserts that ôif it is used appropriately it is probably one of the best interventions you can use to protect yourselfö. So, apparently, in Sridharĺs surreal ecosphere, if people wore masks perfectly all of the time, never tugged and fiddled with them and ľ uh ľ stopped eating and drinking, they would provide some benefit. If only we all lived in a parallel universe.
Sridhar clearly has an emotional attachment to mass masking in the community, perhaps because it chimes with her ideological beliefs about collectivism, the sense that weĺre all in it together and must behave in socially responsible ways. Empirical evidence be damned if it does not support oneĺs political proclivities. This phenomenon is illustrated in Sridharĺs inquiry interview; when the KC states that the science had concluded that public use of face coverings achieved a ônear non-existentö degree of benefit, and then asks her, ôIs this the sort of debate and discussion that you think we should have bypassed?ö Sridhar replies, ôExactlyö. It is reasonable to propose that double standards are on display here; if robust studies had found in favour of masks, Sridhar and her ilk would have been screaming it from the Davos rooftops.
Ignorance around mask harms
Throughout the Covid event, there has been one common factor inherent to all the narratives beseeching us to cover our faces with strips of cloth and plastic: a failure to acknowledge the wide-ranging harms of masking healthy people. This omission ľ due either to ignorance or wilful avoidance ľ is evident once again in Sridharĺs Covid Inquiry testimony. For instance, in her attempt to defend her partisan championing of community masking, she asserts that ôthe cost is slightů so, for me, recommending masks seems a low-cost measure of something easy, like hand-washing, you can tell people to doö.
I sometimes imagine engaging in a prolonged attempt to impress upon Sridhar (or, for that matter, any other pro-mask zealot) the raft of negative consequences (physical, social and psychological) associated with routine masking. And, in this thought experiment, I then envision asking her the question, ôWhat possible harms could there be from masking children and adults in healthcare, education and other community settings?ö I suspect her response might be something like:
There are no appreciable harms to masking [awkward silence]. Okay, well apart from dermatitis, headaches, perpetuating fear, stunting infantsĺ cognitive and emotional development; excluding the hard-of-hearing, evoking fatigue, reducing lung efficiency, tormenting the autistic, increasing falls in the elderly, re-traumatising the historically traumatised, the inhalation of micro fibres, concentration impairment, reducing the quality of healthcare, discouraging patients from attending hospital, impeding school learning, the aggravation of existing anxiety problems, encouraging harassment of the mask exempt, enabling criminals to escape conviction, and polluting our towns and waterways .. [deep breath] what possible harms could there be?
Iĺm sure the Monty Python team would have approved.
*************************************************
Senate votes against vaccine-injured Australians
I am a vaccine-injured Australian, writing under a false name to protect my identity. The reason I do this is because I donĺt want my claim to be affected. No one in power wants to believe me, they just want me to curl up and disappear. I am an inconvenience that threatens the narrative. But there are tens of thousands, maybe even hundreds of thousands, of Australians like me, and we are not going to go gently into the night.
Today, I watched as Gerard Rennick, an LNP Senator for Queensland, moved for an inquiry into the federal COVID-19 Vaccine Injury Claims Scheme. Senator Rennick is one of the only voices that stands up for us. He stands up for us loudly. But his calls for an inquiry were shot down by his colleagues.
According to the parliamentary Hansard, Senator Rennick specifically wanted an inquiry into the schemeĺs eligibility criteria, the time in processing claimantsĺ applications, the differences between the Therapeutic Goods Administrationĺs assessments and specialistsĺ assessments reported in vaccine injury claims, the adequacy of the schemeĺs compensation of claimantĺs injuries, mental health and lost earnings, the risks that inadequate support and compensation for vaccine-related injuries might exacerbate vaccine hesitancy, and other related matters.
In speaking to his motion, Senator Rennick told his colleagues how, in Australia, the government has done a woeful job of acknowledging and compensating those people who it has injured through drugs that it has prescribed. He talked about the victims of thalidomide, and how Prime Minister Anthony Albaneseĺs apology came 60 years too late. He talked about how Australians had suffered in the 1980s when the Red Cross and CSL Limited allegedly infected tens of thousands with AIDS and Hepatitis C. He talked about mesh injuries, and how his uncle had been left blind after taking a sulfa drug. He talked about how the pharmaceutical industry has a history of putting their wallets in front of peopleĺs health. He said that Australians Ĺwere told the vaccine was safe and effective.ĺ He asked, ĹIf we [politicians] arenĺt here to protect the people, what exactly are we here for?ĺ He said that Australians Ĺshould not be made to suffer for following the advice of the government that said they would be protectedĺ.
Later in the debate, another senator said that no one else had spent more time talking to vaccine-injured Australians than Senator Rennick. ĹHe speaks with a good heart and from a place of deep conviction.ĺ And thatĺs right. Senator Rennick does. He talked about and said all the right things. He gave me and all those other vaccine-injured Australians a voice. He was fighting for us, and he was winning.
Then the Albanese governmentĺs chief spokesperson in the chamber, Katy Gallagher, stood up.
Senator Gallagher used her speaking time to gaslight Senator Rennick, describing his views as Ĺirresponsibleĺ. She said that the government would consider the recommendations made to the Finance and Public Administration Legislation Committee, which advocates for a national no-fault vaccine injury compensation scheme. ĹThere is no need for another inquiry,ĺ she finished.
Except thatĺs exactly what the recommendations made to the Finance and Public Administration Legislation Committee demand: a review of the COVID-19 Vaccine Injury Claims Scheme. How can you conduct a review if you canĺt have another inquiry? How, Senator Gallagher, how? She said that the government had only received the report earlier this week, and implied that decisions were being rushed. No, Senator Rennick was just getting on with the job, fighting the good fight. Fighting for us.
When Rennickĺs motion went to a vote, a division was required. The bells were rung. Coalition senators rocked up to support their colleague, as did Malcolm Roberts from One Nation, but it wasnĺt enough. The Labor government, the Greens, Jacquie Lambieĺs mob, and Lidia Thorpe all voted against the motion. It was defeated 24 votes to 31.
This is what the government thinks of us. We are the problem that, in their collective mind, deserves no solution. Australians are dying because they were forced to take an experimental drug and were told that if they didnĺt, they would lose their jobs, their livelihood. They were ridiculed and shamed into submission. At least the Coalition seems to have the courage to admit it got it wrong, and under Senator Rennick wants to try and repair the damage as best it can. Why, now, is the Labor Government so frightened of uncovering the truth?
And I cannot believe that Senator Rennick wonĺt be on the LNPĺs ticket at the next federal election. One of the last blokes with any real guts in Canberra, prepared to stand up to the powerful, has been, like we have, shoved aside.
This is a dark day for Australia, but itĺs just another day in the last four years for me, for all those Australians injured by the Covid vaccines.
https://www.spectator.com.au/2024/03/senate-votes-against-vaccine-injured-australians/
*************************************************21 March, 2024
New Canadian vaccine works
As SARS-CoV2 evolves into more distant Omicron variants, companies continue to invest in research and development and potentially vie for lucrative government contracts for future COVID-19 vaccine deals. In this context, the Canada based Providence Therapeutics mRNA platform appears to support the acceleration of next-generation COVID-19 vaccine candidates.
Researchers affiliated the clinical-stage mRNA platform company developing vaccines for cancers and infectious disease, report on a study comparing their investigational mRNA vaccine with the Pfizer-BioNTech COVID-19 vaccine BNT162b2 (Comirnaty). When considering this approach to mRNA vaccine development the company touts its ôdynamic and adaptable responses, emphasizing the importance of sustained vaccination strategies.ö
How did the Canadian companyĺs experimental vaccine targeting COVID-19 compare against Pfizer-BioNTech BNT162b2 in a Phase 2 clinical trial?
With results of this study (NCT05175742) published in Nature Scientific Reports, the study team based out of Canada reports on the results of the head on comparison study leveraging trial sites in Canada and South Africa.
The Study
In this investigation, the sponsor-funded study looks at their COVID-19 vaccine called PTX-COVID19-B mRNA Humoral Vaccine, developed to prevent COVID-19 in a general population. Importantly, the Pfizer-BioNTech vaccine does not stop viral transmission but reduces the probability of morbidity and mortality.
For comparison of the vaccines, the studyĺs protocol was designed to produce the data to evaluate the safety, tolerability, and immunogenicity of PTX-COVID19-B compared to Pfizer-BioNTech COVID-19 vaccine in healthy seronegative adults aged 18 to 64.
An observer-blind, double-dummy, randomized immunobridging phase 2 study, the researchers compared the immunogenicity induced by two doses of 40 ?g PTX-COVID19-B vaccine candidate administered 28 days apart, with the response induced by two doses of 30 Ág Pfizer-BioNTech COVID-19 vaccine (BNT162b2), administered 21 days apart, in Nucleocapsid-protein seronegative adults, again ranging in age from 18ľ64 years.
The study team reports that both vaccines were administrated via intramuscular injection in the deltoid muscle. Two weeks after the second dose, the neutralizing antibody (NAb) geometric mean titer ratio and seroconversion rate met the non-inferiority criteria, successfully achieving the primary immunogenicity endpoints of the study. PTX-COVID19-B demonstrated similar safety and tolerability profile to BNT162b2 vaccine.
Importantly, a non-inferiority trial is a study that determines if a new treatment is not worse than an active treatment it is being compared to. These trials are used when a placebo (an inactive treatment) cannot be used, or when the incremental benefits of newly developed treatments may be only marginal over existing treatments, which appears to be the case here.
While NAb with lowest response was detected in subjects with low-to-undetectable NAb at baseline or no reported breakthrough infection, the study investigators also found that the study result demonstrates induction of cell-mediated immune (CMI) responses by PTX-COVID19-B.
Cell-mediated immunity (CMI), also known as cell-mediated immune response or cell-mediated immune defense, is a crucial aspect of the immune system's defense mechanism. It involves specialized cells, primarily T lymphocytes (T cells), which directly attack and destroy infected or abnormal cell
Summary
According to the entry, the candidate PTX-COVID19-B demonstrated favorable safety profile along with immunogenicity similar to the active comparator BNT162b2 vaccine.
**********************************************
Now That Puberty Blockers Have Been Banned, itĺs Time to Ban Covid Vaccines for Children Too
Puberty blockers have finally been banned in the U.K. The decision came after an independent review of services for children under 18 and a sharp rise in referrals to the Gender Identity Development Service run by the Tavistock and Portman NHS Foundation Trust, which is closing at the end of March.
ôWe have concluded that there is not enough evidence to support the safety or clinical effectiveness of puberty-suppressing hormonesö an NHS spokesperson told the Telegraph on March 12th 2024.
MPs and media personalities have come out in support of this move. But in reality, most of them have remained silent on this issue up until now. It has previously been considered too politically sensitive and controversial to comment on, with the threat of being branded a Ĺtransphobeĺ or Ĺbigotĺ no doubt playing a significant role in their collective silence. Nonetheless, I have yet to meet a single person, outside of social media, who agrees that puberty blockers are either ethical or safe. Thankfully, strong and courageous voices, such as J.K. Rowling, Allison Pearson, Molly Kingsley and Jordan Peterson have been calling out the dangers of this practice from the start. They are now clearly vindicated.
When the issue is stripped back to its essence, puberty blockers have been banned on the basis of long established medical ethics. Specifically, that children should never be given a medical intervention which they do not need and which poses known and serious risks to them ľ a view which before 2020 would have been the reasonable position to take. Indeed, to argue otherwise would have been regarded as extreme. The factor which changed after 2020 was the rollout of the Covid vaccines to children. Seemingly overnight, medical ethics was suspended and inverted in favour of pushing ahead with the vaccine rollout. However, if we apply the same principles behind the banning of puberty blockers to the Covid vaccines, they would also be banned for children with immediate effect.
The Covid vaccine rollout to children has always been controversial. Consider:
Covid vaccinations were not recommended by the Joint Committee on Vaccination and Immunisation (JCVI) for under-16s, a decision overridden by the Chief Medical Officers in England, Wales, Scotland and Northern Ireland.
When Matt Hancock was Health Secretary, he stated in Parliament that the Covid vaccines were for the adult population only. He said that children would not be offered the vaccine because it had not been tested on children and that they were at low risk from Covid. Despite this, he then supported the rollout to the nationĺs children.
There are still no long-term safety data for the Covid vaccines (and at the time of the rollout to children, incomplete short-term and no medium-term safety data).
Covid vaccines pose known and very serious risks (these include potentially fatal myocarditis, pericarditis etc.) Tragically, there have also been coroner confirmed deaths caused by the Covid vaccines.
A child can still catch and spread Covid when vaccinated against the virus.
Healthy children are at extremely low risk of serious illness from Covid, so the risks posed by the vaccines outweigh any possible benefit for a child.
When Sajid Javid was Health Secretary, he stated that 12 to 15 year-old children would have the final say on whether or not to receive the Covid vaccine. Children were told that they were allowed to override their parentsĺ decision. This remains, in my opinion, the most egregious act of the entire pandemic.
The Government chose Pfizer, the pharmaceutical company with a long history of criminal and medical negligence (and which paid the biggest criminal fine in U.S. history) as the company to provide the Covid vaccine for our children. This really should have been a red flag from the start.
One of the most controversial points was the decision by the U.K. Government to shut down its own Ethics Committee when its members raised serious concerns about the Covid vaccine rollout to children.
Like puberty blockers, the general public appears to have been opposed to the Covid vaccine rollout to children. In the end, 89.4% of five to 11-year-olds did not receive a single Covid vaccine or booster. This is despite a multi-million pound marketing campaign directed at children and their parents. Over 50% of the 12-15 year old cohort did not receive a single dose either.
The evidence keeps stacking up against the Covid vaccines
MPs have said they believe the MHRA were aware of heart and clotting issues caused by the Covid vaccines in February 2021 but did not highlight the problems for several months. The all-party parliamentary group (APPG) on pandemic response and recovery raised ôserious patient safety concernsö, claiming that ôfar from protecting patientsö the regulator operates in a way that ôputs them at serious riskö. Some 25 MPs across four parties wrote to the Health Select Committee asking for an urgent investigation.
The group also warned that the MHRA Yellow Card reporting system ľ which encourages patients and doctors to flag-up medicine side effects ľ ôgrosslyö underestimates complexities, and in some instances picks up just one in 180 cases of harm.
MPs and peers have also accused the Health Secretary of withholding data that could link the Covid vaccine to excess deaths, and criticised a ôwall of silenceö on the topic. A cross-party group has written to Victoria Atkins to sound alarm about the ôgrowing public and professional concernsö at the U.K.ĺs rates of excess deaths since 2020.
With the growing evidence that something is seriously amiss with the Covid vaccines, surely we should stop giving them to our children? Currently within the U.K., children who are considered vulnerable (including those with Autistic Spectrum Disorder and ADHD) and those living with clinically vulnerable adults are eligible for the vaccine. It is also possible for parents to privately purchase the Covid vaccine for their children if they are 12 years old or over. In light of the ban on puberty blockers, it makes sense to apply this thinking to the Covid vaccines too.
Things will change when members of the public speak up
Being critical of puberty blockers will become the accepted narrative now that they have been banned. Members of the public, media personalities and politicians will begin to openly express this position (which has always been the majority view). However, we need to get to a point when people begin to express opinions which they genuinely hold but are still considered controversial. Expressing lawful opinions about sensitive topics, particularly when it comes to safeguarding children against harm, should be encouraged and not vilified.
All of the safeguarding training across workplace sectors is easily dismantled and destroyed in the face of moral cowardice. As a former headteacher, with 30 yearsĺ experience within the education sector, I had to attend annual safeguarding training which laid out what an education professional must do when he or she has concerns about a child. The training always highlighted examples in which entire organisations have been complicit in widespread abuse.
We are told that it is not just the perpetrators of the abuse who are accountable. Those who are not directly involved in the abuse, but who remain silent about it, are equally accountable under law. These individuals, woefully lacking in moral courage, place their self-preservation ahead of the needs of the children in their care. It is also a serious breach of their legal duty to safeguard children against harm.
Of course, cancel culture, as well as employers evangelised by whatever the latest thing happens to be, inhibits free speech. If an opinion goes against the current narrative, employees are likely to be attacked for expressing it. Whether that be criticism of puberty blockers, the Covid vaccines, climate alarmism, drag queen storytime or anything else. Expressing lawful opinions about controversial and politically sensitive topics will almost always result in some sort of attack. However, we must draw a line when it comes to safeguarding children against harm.
As the only U.K. headteacher to publicly express concerns about lockdowns, masking kids and the Covid vaccines for children, I have experienced multiple attacks and personal losses. This is why I am now taking my former employer, East Sussex County Council, to court. In the end, expressing my valid concerns in a lawful and moderate manner cost me my career. My employer tried to silence me through the complaints and investigation process, but I continued to express my concerns. I was fulfilling my legal and moral duty in doing so. My philosophical belief in the importance of critical thinking, freedom of speech and safeguarding children underpins my case. It is predicted to set an important legal precedent for free speech in the workplace and has gained the overwhelming support of the public, high-profile free speech advocates and the Daily Telegraph.
But it neednĺt result in expensive court cases and conflict if everyone expressed their lawful opinions about the things which matter. The ban on puberty blockers is a fantastic development in the battle to protect our children, but those who were silent about it are partly responsible for the delay. This abhorrent medical intervention should have been banned long ago. The same principles applied to the ban on puberty blockers should now be applied to the Covid vaccines for children. Children do not need this medical intervention, which is ineffective and known to cause harm. The general public is clearly in agreement so the time to speak up about it is now. Silence should never be an option when safeguarding children against harm.
*************************************************
20 March, 2024
Murthy v. Missouri Puts Government Censorship on Trial
On Monday, the Supreme Court will hear arguments in Murthy v. Missouri, formerly Missouri v. Biden, the president whose administration has been accused of strong-arming Big Tech to remove “objectionable posts.” The attorneys general of Missouri and Louisiana, joined by doctors such as Jay Bhattacharya of Stanford, argue that the administration censored dissenting speech on COVID-19 and other policies by pressuring tech platforms to remove or restrict posts.
Consider this account from Martin Kulldorff, former professor of medicine at Harvard and co-author of the Great Barrington Declaration (GBR) with Dr. Bhattacharya and Oxford University’s Sunetra Gupta, a leading infectious-disease epidemiologist. The GBR, signed by thousands of medical scientists, advocated an approach to the pandemic similar to the one taken by Kulldorff’s native Sweden, which declined to shut down schools.
Kulldorff recalls that although Sweden had the lowest excess mortality among major European countries and “despite being a Harvard professor, I was unable to publish my thoughts in American media. Twitter (now X) put me on the platform’s Trends Blacklist.” Twitter did the same to Dr. Bhattacharya.
“Seeking to prop up Anthony Fauci and the lockdown policies he promoted in response to the COVID-19 pandemic,” the plaintiffs explain, “Twitter (and other Big Tech companies) intentionally blacklisted, censored, suppressed, and targeted the GBD and its signers.”
National Institutes of Health (NIH) director Francis Collins smeared the GBD authors as “fringe epidemiologists,” but they were far more qualified than Collins, a “lab scientist with limited public-health experience,” according to Kulldorff. Fauci, longtime boss of the National Institute of Allergy and Infectious Diseases, is a nonpracticing physician whose bio shows no advanced degrees in molecular biology or biochemistry. The government’s white-coat supremacists were causing extensive damage, and the GBD scientists called them out.
“It was also clear that lockdowns would inflict enormous collateral damage,” notes Kulldorff, “not only on education but also on public health, including treatment for cancer, cardiovascular disease, and mental health. We will be dealing with the harm done for decades. Our children, the elderly, the middle class, the working class, and the poor around the world—all will suffer.”
As the ousted Harvard professor explains, “The pursuit of truth requires academic freedom with open, passionate, and civilized scientific discourse, with zero tolerance for slander, bullying, or cancellation.” That sort of activity has been going on at Facebook for some time.
In 2018, in his first public testimony before Congress, CEO Mark Zuckerberg admitted that Facebook was collaborating with the investigation of President Trump by former FBI director Robert Mueller. The FBI had interviewed some Facebook employees, but Zuckerberg would not say who they were “because our work with the special counsel is confidential.”
When Sen. Ted Cruz asked Zuckerberg if Facebook was a “neutral forum,” the CEO seemed puzzled by the concept. Sen. Cory Gardner asked if the government had ever demanded that Facebook remove a page from the site. “Yes, I believe so,” said Zuckerberg. He did not reveal the content of the page or when the removal had taken place.
Joe Biden has accused Facebook of “killing people” with vaccine misinformation. From the ordeals of Kulldorff, Bhattacharya and others, it’s now clear that the Biden administration was peddling misinformation, slandering the GBD scientists, and blocking them from setting forth the truth to the widest possible audience.
“In an environment where just about every decision tech platforms make becomes highly politicized,” one article previewing Murthy v. Missouri explains, “lawmakers on both sides of the aisle have grown accustomed to making pointed—if, often empty—threats at Big Tech. Now, the Supreme Court will decide just how far those threats can go.”
Murthy v. Missouri aside, it’s clear that white-coat supremacy and government censorship are incompatible with a free, safe, and healthy society.
**************************************************
Mandatory lockdowns had almost no benefit—but did significant economic and health-related damage
Four years ago this week Vice President Mike Pence announced the White House’s “15 days to slow the spread” campaign. What followed was the unprecedented use of lockdowns, school closings and other sweeping measures to mitigate Covid-19.
Four years later, we know what many of us suspected then: None of those policies were successful, and many were gravely damaging.
The Covid health benefits of mandatory lockdowns were tiny. Lockdowns in the U.S. prevented between 4,000 and 16,000 Covid deaths. In an average year 37,000 Americans die from the flu, according to the Centers for Disease Control and Prevention. Lockdowns also failed to reduce infections more than a trivial amount, in part because people voluntarily alter their behavior when a bad bug is in the air. Coercive government policies generated few benefits—and massive costs.
Public-health agencies exacerbated the damage by failing to keep their heads and follow standard pandemic-management protocols. Before 2020, it was recognized that communities respond best to pandemics when government measures are only minimally disruptive. During Covid, however, officials junked that practice by green-lighting restrictive practices and intentionally stoking fear. That response overlaid enormous economic, social, educational and health harms on top of those caused by the virus.
Those harms are captured, in part, in excess deaths—the number beyond what would have been expected without a pandemic. Non-Covid excess deaths from lockdowns, the shutdown of non-Covid medical care, and societal panic are estimated at nearly 100,000 between April 2020 and at least the end of 2021. The number of lockdown and societal-disruption deaths since 2020 is likely around 400,000, as much as 100 times the number of Covid deaths the lockdowns prevented.
The best measure of health performance during the pandemic is all-cause excess mortality, which captures the overall number of deaths relative to the expected level, encompassing Covid and lockdown-related deaths. On this measure Sweden—which kept most schools open and avoided strict lockdown orders—outperformed nearly every country in the world.
A recent study published in the Proceedings of the National Academy of Sciences found that the U.S. “would have had 1.60 million fewer deaths if it had the performance of Sweden, 1.07 million fewer deaths if it had the performance of Finland, and 0.91 million fewer deaths if it had the performance of France.” In America, states that imposed prolonged lockdowns had no better health outcomes when measured by all-cause excess mortality than those that stayed open. While no quantifiable relationship between lockdown severity and a reduction in Covid health harms has been found, states with severe lockdowns suffered significantly worse economic outcomes.
Closing hospitals and cutting off access to non-Covid healthcare generated a fear of entering medical facilities. That was a profound mistake, as was encouraging the false belief that hospitals were too busy to treat people who needed care. Healthcare utilization rates were at low levels between 2020 and 2022. In spring 2020, nearly half of the nation’s some 650,000 chemotherapy patients didn’t get treatment, and 85% of living organ transplants weren’t completed. One study found that there were 35.6% fewer calls for cardiac emergencies after March 10, 2020, compared with the year prior. Emergency-room visits were down between 40% and 50%, according to an estimate in May 2020. That doubtless contributed to observed non-Covid excess deaths and may continue to do so, as Americans suffer from undetected cancers and other long-term conditions. Healthcare uptake is still lower than pre-pandemic levels.
The economic costs of lockdowns were also staggering. According to the Bureau of Labor Statistics, as many as 49 million Americans were out of work in May 2020. This shock had health consequences. A National Bureau of Economic Research study found that the lockdown unemployment shock is projected to result in 840,000 to 1.22 million excess deaths over the next 15 to 20 years, disproportionately killing women and minorities.
Perhaps the worst policy error was prolonged school closings. Learning loss for children, especially in poor families, is already showing up in reduced standardized-test scores. These losses will affect earnings for decades. By one estimate today’s children will lose $17 trillion in lifetime earnings owing to school closings. They may also suffer shorter life expectancy, which is linked to income and educational attainment.
While school closings had no offsetting public-health benefits, the attendant isolation led to massive increases in psychiatric illness, self-harm, obesity and substance abuse. Healthy children were always at vanishingly small risk from Covid, and nearly all of them were infected at some point anyway, according to CDC data. Like a regressive tax, these harms were severest for lower-income and minority students.
One result of the government’s Covid response is that Americans have lost faith in public-health institutions. To earn back their confidence, Congress and the states should rewrite their statutes regarding public-health emergencies. Legislatures should place strict limitations on the powers conferred to public-health executives, in addition to implementing sunset clauses that require legislative majorities to extend them. Congress should likewise set term limits for all senior positions in U.S. health agencies.
The CDC, the Food and Drug Administration and the National Institutes for Health should be fully transparent about their deliberations. They should publish transcripts of their formal discussions on digital forums for public consumption. Congress should also restate that the CDC’s guidance is strictly advisory and that the agency doesn’t have power to set laws or issue mandates. The U.S. should halt all binding agreements with the World Health Organization until it also enhances transparency and accountability.
Most important, these institutions must acknowledge that lockdowns, school closings and mandates were egregious errors that won’t be repeated. Until they do, the American people should continue to withhold their trust.
https://www.wsj.com/articles/covid-lessons-learned-four-years-later-596a9fa9
*************************************************19 March, 2024
Report claims Covid-19 lab leak theory Ĺmore probableĺ than natural occurrence
What was once considered a far-fetched conspiracy theory has now been floated as a ômore probableö answer to the million dollar Covid-19 question.
The origins of Covid-19 have been pontificated on by millions around the world after the first wave exploded through Wuhan, China in 2019.
The US National Library of Medicine claimed the virus that turned planet Earth on its head originated from pangolin samples ôobtained by anti-smuggling operations in the Guangdong province of Chinaö.
But sceptics have been highly critical of the assumption the virus, which was highly infectious to humans, naturally developed in the wild.
The Lancet, another major medical journal, boldly proclaimed that those suggesting the virus originated from a laboratory were attempting to ômanipulate public opinion with political languageö.
ôPeer-reviewed evidence available to the public points to the hypothesis that SARS-CoV-2 emerged as a result of spillover into humans from a natural origin,ö the Lancet published in 2023.
But now, a major scientific paper led by Australian pandemic expert Professor Raina MacIntyre suggests that a lab leak is actually ôequally or more probableö than Covid-19 springing from nature.
The paper, featuring scientists from the Kirby Institute at the University of NSW, says that while a lab leak theory is plausible, the true origin of the pandemic may never be confirmed.
The research used the Grunow-Finke tool, an epidemiological risk scoring method, contrasting with the genetic analysis methods more commonly used to investigate the virusĺs origins.
ôAn unnatural origin of SARS-COV-2 is plausible, and our application of the Grunow-Finke tool suggests it is equally or more probable than a natural origin, although both remain possible,ö the researches wrote.
ôThe gathering of intelligence may include open source, signals or satellite intelligence, political factors, as well as other Ĺdetective workĺ to piece together the complex question of the origin of SARS-COV-2.
ôThis would include full records of viruses housed at the relevant laboratories, of experiments conducted, and records of accidents and illness among staff. The question of origin cannot be answered solely by phylogenetic analysis, as viruses resulting from gain-of-function research using serial passage in an animal model cannot easily be distinguished from naturally emerged ones.ö
This analysis is presented against a backdrop of widespread dismissal of the lab leak hypothesis in scientific circles and by the World Health Organisation, which deemed a leak from the Wuhan Institute of Virology ôextremely unlikelyö.
The study analysed various factors, including the peculiar biological characteristics of SARS-CoV-2, its rapid human-to-human transmission rate, and unusual actions at the Wuhan Institute of Virology prior to the outbreak, such as military control takeover and removal of a large virus database from public access.
The paperĺs findings, suggesting a 68 per cent likelihood of an unnatural origin of SARS-CoV-2 based on the modified Grunow-Finke tool, contrast sharply with other scientific opinions and WHO conclusions.
The research has been criticised by some international scientists, including Alice Hughes from the University of Hong Kong, who labelled the analysis method as potentially ôdangerous and misleadingö due to its subjective nature and reliance on conjecture.
As the world emerges from one of the most destabilising periods in recent history, more and more information about the potential cause of the pandemic has risen to the surface.
In November 2023, a whistleblower came forward to claim CIA analysts who favoured the lab leak theory were bribed to change their position.
The bribe was allegedly made to take the focus off China and the Wuhan Institute of Virology.
The National Intelligence Councilĺs Director for Global Health Security, Adrienne Keen, worked as an independent consultant for the WHO from 2016.
Former Acting Assistant Secretary of State Thomas DiNanno said that Ms Keene tried to push Covid-19 was a natural occurrence, rather than a lab leak.
ôI had found out that apparently she was an outside adviser also to the World Health Agency ľ they are a political agency, they are a UN agency,ö Mr DiNanno said.
ôItĺs just not appropriate to do work for a foreign power and that would include in the United Nations.ö
A few months prior, a report claimed that Covid-19ĺs ôpatient zeroö was a Wuhan scientist carrying out experiments on souped-up coronaviruses,
According to the report, the scientist, Ben Hu, was conducting risky tests at the Wuhan Institute of Virology with two colleagues, Ping Yu and Yan Zhu.
Itĺs understood all three fell ill with Covid-like symptoms and needed hospital care weeks before China disclosed the virus outbreak to the world.
A bombshell report by journalists Michael Shellenberger and Matt Taibbi alleged the scientists were experimenting with coronaviruses when they became sick in 2019.
Many experts and intelligence officials have long suspected scientists at the lab accidentally spread Covid-19 during so-called ôgain of functionö experiments on bat coronaviruses.
The naming of ôpatient zeroö could be the so-called smoking gun ľ adding to mounting circumstantial evidence of a lab leak.
Itĺs not clear who in the US government had the intelligence about the sick lab workers, how long they had it, and why it was not shared with the public.
Jamie Metzl, a former member of the World Health Organisation advisory committee on human genome editing, described it as a possible ôgame changerö.
ôItĺs a game changer if it can be proven that Hu got sick with Covid before anyone else,ö he said.
ôThat would be the Ĺsmoking gunĺ. Hu was the lead hands-on researcher in (virologist Shi Zhengliĺs) lab.ö
***********************************************
UK: Up to 20,000 prostate cancer diagnoses could have been missed during the pandemic, research suggests
Up to 20,000 diagnoses of prostate cancer could have been missed during the pandemic, research suggests.
Analysis of 24million patient records since 2020 found tens of thousands of men have missed potentially life-saving cancer diagnoses.
The study by the University of Surrey and the University of Oxford said there was 'unprecedented disruption' in the diagnosis of cancer with a drop in urgent referrals from GPs, caused by difficulties accessing care and longer waiting times.
They analysed prostate cancer incidence between January 2015 and July 2023 using data representing 40 per cent of the country. This revealed a 31 per cent drop in diagnoses of prostate cancer in 2020 and 18 per cent in 2021, returning to normal in 2022.
When extrapolated across the country, there were 19,800 fewer cases, according to the findings published in the British Journal of Urology International.
Lead author Dr Agnieszka Lemanska, of the University of Surrey, said: 'Understandably, during the pandemic, resources and attention in healthcare systems shifted towards preventing and managing the virus.
'It is important that we learn the lessons from the pandemic. However, to do this, we need to understand the scale of how diagnosis rates were impacted during this time.'
*************************************************
18 March, 2024
mRNA Experts acknowledge many faults in mRNA vaccines
But they still seem to believe that the vaccines helped on balance. Most deaths were among the elderly, who probably died WITH rather than FROM Covid. Among the under-65s, most infections were minor. A few lives may have been saved by the vaccines but some were lost from vaccine effects too
A trio of experts from one of the birthplaces of mRNA breakthroughs represented by Drew Weissman, MD, PhD Perelman School of Medicine, University of Pennsylvania, and along with Katalin Kariko, winner of the Nobel Prize in Physiology or Medicine in 2023 for their role in driving mRNA-related discovery directly influencing the development of the PfizerŚBioNTech COVID-19 vaccine (BNT162b2) discuss the need to look at mRNA technology, beyond the COVID-19 vaccines.
In a way, a code word to acknowledge that these products in the form delivered to the world as a mass countermeasure/immunization scheme during a global pandemic are not ready for more refined therapeutic delivery. Put another way the products as represented by the vaccines are by no means ready for prime time! Why? One of the true authorities on the subject of mRNA, Weissman and University of Pennsylvania colleagues, point out in their recent paper published in The Lancet problems, or challenges ongoing with mRNA stability, duration of expression, targetability, and the like, but also introduces scientific advances to harden these products. These products were rushed to market in the pandemic. Key preclinical steps such as pharmacodynamics were all but bypassed due to the exigencies of the time. As a deadly virus spread, government health agencies and industry decided that acceleration of mRNA vaccine delivery for mass immunization was acceptable.
Yet because of the emergency conditions and the medical establishmentĺs declaration that the vaccines saved millions of lives, any externalities continue to be swept under the carpet of history. And these are externalities that derive from the gaps called out by one of the most notable authorities on the topic of mRNA technology. Advancing this medicinal technology in more refined therapeutics necessitates improvements they discuss in their paper. The good news, industry is quietly capitalizing on advancements in science to stabilize these products. The bad news, any externalities adversely affecting what is likely a relatively small percentage of the masses during the pandemic donĺt exist according to the medical establishment. Is human suffering a consequence of advancement?
Declaring that the recent COVID-19-driven advancements ushered in a new era in medicine powered by mRNA-based therapeutics, ôthe rapid, potent, and transient nature of mRNA-encoded proteinsö less any nucleus penetration or risk of genomic integration positions mRNA-based medicine as ôdesirable tools for treatment of a range of diseases, from infectious diseases to cancer and monogenic disorders (inheritance of a single gene mutations).
Yet this view evades over some fundamental challenges that the medical research establishment will not come out and admit publicly! At least in a minority of cases, for example, the spike protein generated by the mRNA does not just flush out of the system as declared by the boosters. Peer-reviewed study after peer-reviewed study finds evidence of the spike protein distribution sending the potentially toxic protein to various tissues or organs in the human body. This has become fact yet the medical research establishment will not accept this reality, at least not yet.
Or perhaps they have and experts such as Dr. Drew Weissman, the American physician-immunologist known for this contributions to RNA biology, whose work underlies the development of the mRNA vaccines of BioNTech (Pfizer), does perhaps acknowledge the need to advance the technology in this latest piece published in The Lancet.
While he and Penn-based colleagues declare in their recent paper, ôThe rapid pace and ease of mass-scale manufacturability of mRNA-based therapeutics supported the global response to the COVID-19 pandemic,ö they explicitly acknowledge that ôchallenges remain with regards to mRNA stability, duration of expression, delivery efficiency and targetability.ö Acknowledging and overcoming these fundamental challenges, an admission in many ways, are absolutely vital before any broadening of applicability for mRNA therapeutics can happen.
Put in simple terms the trio, rightly considered an authority on the topic, argue in this latest entry that itĺs not prime time for mRNA technology!
But hold on, didnĺt we just inject hundreds of millions of people worldwide with mRNA vaccines? Yes, of course, and that was an emergency use authorization scenario in an emergency setting. And while the jabs were ultimately approved by the Food and Drug Administration (except now for children 6 months to 11, which are still investigational), driving their logic is the assumption that the benefits given the COVID-19 pandemic outweighed any costs or externalities, which medical authorities and regulators resist any acknowledgment.
Of course, the evidence of these externalities exists in persons that combat ongoing issues, injuries derived from the mass immunization program. TrialSite has amassed more than enough evidence along with partner React19, the largest COVID-19 vaccine injury advocacy group worldwide.
TrialSiteĺs founder, Daniel OĺConnor, shared, ôThis most recent piece in The Lancet represents yet another admission as to the reality that itĺs not prime time yet for the mRNA therapeutic technology.ö The TrialSite founder said, ôYou could not find a better, more authoritative source than Dr. Weissman, who, along with Katalin Kariko, received the Nobel Prize in Physiology or Medicine in 2023 for the discoveries of these two leading to the mRNA technology today as we know it.ö
TrialSite has tracked a series of papers and studies now representing authoritative figures in science who come forth via academic papers discussing the gap between the existing platform in use, billions of doses administered, and the needs for better stability, efficient delivery, and targetability, as Weissman and colleagues postulate.
For example, TrialSite recently reported on the ex-Moderna scientists and the Northeastern University professor that recently had a similar paper published.
See the TrialSite piece based on the authored by four ex-Moderna scientists and a Northeastern University professor, the paper calls attention to serious limitations in the existing mRNA technology now on the market. See ôBombshell? Ex-Moderna Preclinical Scientists Acknowledge Serious Safety Concern with Current mRNA Technology..ö
Weissman and colleagues acknowledge the ongoing need to learn ôrapidlyö from the growing number of both preclinical and clinical trials testing mRNA-based therapeutics and vaccines.
The goal: to optimize what essentially in the minds of the authors are a proven medical technology, based on what Weissman and colleagues breakdown as advances in mRNA technology, many overlapping with those discussed by the ex-Moderna scientists and in select other papers published in TrialSite.
How are these advancements being used in Immunotherapeutics, protein replacement therapy, and genomic editing? How is targetability improving in that scientists can, with more predictability, deliver mRNA to ôdesired specific cell types and organs?ö
These breakthroughs, or better, incremental advancements are what is needed to validate the ôdevelopment of the next generation of targeted mRNA therapeutics.ö
Behind The Lancet paywall, we must respect their boundaries, as we have our own for economic sustainability, so for those tracking these trends the Weissman piece most certainly should be studied.
But here at TrialSite, we think itĺs fair and important to ask about those gaps, the deficiencies in the mRNA technology that were clearly part of the emergency countermeasure product administered by over a billion people. Considering externalities in what, in essence, was a declared war against a pathogen, why is there such resistance to recognize and accept publicly what one of the true inventors of the technology has acknowledged?
*************************************************
17 March, 2024
Catching Covid has made people less intelligent - with severe infections reducing IQ the most, new study suggests
14 March, 2024
‘Laissez-Faire’ Sweden Had the Lowest COVID Mortality in Europe
Gore Vidal once said “I told you so” are the four most beautiful words in the English language.
Perhaps this is why it’s difficult to resist sharing new data that show how Sweden’s much-maligned pandemic response was right after all.
For those who’ve forgotten, Sweden was excoriated by corporate media and US politicians for its lighter-touch Covid-19 strategy. Many were downright hostile to the Swedes for refusing to shutter schools, lock down businesses, and ramp up police to enforce mandates.
Here’s a sample of headlines:
• “Why the Swedish Model for Fighting COVID-19 Is a Disaster” (Time, October 2020).
• “The Inside Story of How Sweden Botched Its Coronavirus Response” (Foreign Policy, December 2020).
• “Sweden Stayed Open and More People Died of Covid-19, but the Real Reason May Be Something Darker” (Forbes, 2020).
• “Sweden Has Become the World’s Cautionary Tale” (New York Times, July 2020).
• “I Just Came Home to Sweden. I’m Horrified by the Coronavirus Response Here” (Slate, April 2020).
This is just a taste of the reactions against Sweden in 2020. By opting to allow its 10 million citizens to continue living relatively normal lives, Sweden was, in the words of The Guardian, leading not just Swedes but the entire world “to catastrophe.”
Even then-president Trump got in on the action of smacking Sweden around.
“Sweden is paying heavily for its decision not to lockdown,” the tweeter-in-chief warned.
Despite the foreboding rhetoric, the worst-case predictions for Sweden never materialized. In fact, they were not even close.
In March 2021, it was apparent that Sweden had a lower mortality rate than most European nations. The following year, Sweden boasted one of the lowest mortality rates in Europe.
By March 2023, Sweden had the lowest excess death rate in all of Europe, according to some data sets. And though some weren’t ready to admit that Sweden had the lowest excess mortality in all of Europe, even the New York Times, which had mocked Sweden’s pandemic strategy, conceded that the nation’s laissez-faire approach was hardly the disaster many had predicted.
More recently, Danish economist Bj°rn Lomborg shared a statistical analysis based on government data from all European countries from January 2020 to August 2022. The study demonstrated that Sweden had the lowest cumulative age-standardized mortality rate in all of Europe in that period.
“Across Europe, Sweden saw [the] lowest total death during and after Covid,” Lomborg said on X (formerly Twitter).
One Economic Fallacy to Rule Them All
Lomborg’s analysis provides yet more evidence that the Covid state was a disaster.
Some will say, How could we have known?
The harsh truth is that some of us did know. In March 2020, I warned that government “cures” for Covid-19 were likely to be worse than the disease itself. The following month, I argued that Sweden’s laissez-faire policy was likely to be a more effective policy than the hardline approach favored by other nations.
I wrote these things not because I’m a prophet, but because I’ve read a bit of history and understand basic economics.
History shows that collective responses during panics tend not to end well, and economist Antony Davies and political scientist James Harrigan explained why near the beginning of the pandemic.
“In times of crisis, people want someone to do something, and don’t want to hear about tradeoffs,” the authors noted. “This is the breeding ground for grand policies driven by the mantra, ‘if it saves just one life.’”
The thing is, tradeoffs are real. Indeed, economics is largely a study of them. When you choose one thing, you give up another; and we evaluate outcomes based on what we get versus what we gave up. We call this opportunity cost.
Throughout most of the pandemic, however, there were those who didn’t want to pay any attention to opportunity costs or the unintended consequences of government lockdowns—and they were legion.
This is the great economic fallacy Henry Hazlitt warned of decades ago.
Hazlitt, the author of Economics in One Lesson, claimed that overlooking the secondary consequences of policies accounted for “nine-tenths” of the economic fallacies in the world.
“[There is] a persistent tendency of men to see only the immediate effects of a given policy,” he wrote, “and to neglect to inquire what the long-run effects of that policy will be.”
This was the fatal flaw—quite literally—of the Covid state. Its engineers didn’t realize they were not saving lives, but trading lives (to borrow a turn of phrase from Harrigan and Davies).
Lockdowns weren’t scientific and proved ineffective at slowing the spread of Covid, but even if they had worked, they came with severe collateral damage: cancer screenings plummeted, drug use surged, learning was lost, and global poverty exploded. Depression and unemployment skyrocketed, businesses went bankrupt, and high inflation arrived. Babies were denied heart surgery because of travel restrictions, youth suicides increased…the list goes on and on.
The dark truth is that lockdowns were not based on science and came with a rather unfortunate side effect: they killed people.
‘A Giant Experiment’
The secondary consequences of lockdowns and other non-pharmacological interventions (NPIs) did irreparable harm to humans that will be experienced for decades to come.
In the words of New York magazine, lockdowns were “a giant experiment” that failed.
Sweden’s top infectious disease expert, Anders Tegnell, was one of the few people to understand that lockdowns would probably not work. And though Tegnell is not a professional economist, he seemed to understand the lesson of secondary consequences better than many economists.
“The effects of different strategies, lockdowns, and other measures, are much more complex than we understand today,” he told Reuters in 2020, when his strategy was under fire.
By understanding this basic economic principle and having the courage to stand by his convictions, Tegnell was able to avoid the pernicious effects of lockdowns, a policy that seduced so many central planners.
Today, many more people in Sweden are alive because of it. And Anders Tegnell should not be shy in saying, “I told you so.”
https://catalyst.independent.org/2024/03/12/laissez-faire-sweden-mortality/
*********************************************Court Strikes Down $3,000 Fine for Person Trying to Leave City During Pandemic
The NSW Supreme Court has found that a $3,000 fine for leaving Greater Sydney without a permit in 2021 was unlawful, casting doubt on the validity of around 30,000 similar fines issued during the pandemic.
This is the second such ruling.
The state’s Revenue NSW, however, says it will not withdraw the fines and, will instead, treat each one on a “case-by-case basis,” likely meaning those fined will need to argue their case with the government and potentially take the matter to court.
The case centred on a $3,000 fine imposed on Angelika Kosciolek for leaving Greater Sydney in 2021. She was homeless and made plans to travel to South Australia after being offered accommodation there.
But Justice Desmond Fagan said fines issued during COVID-19 must pass the “bare minimum test,” established in a 2022 Supreme Court ruling. That ruling said that for a fine to be valid, the penalty notice must clearly state the relevant Act, and the provision related to the offence.
Ms. Kosciolek’s fine was found to have not passed that test, and the Redfern Legal Centre (RLC) said most COVID-19 fines also failed to precisely state which laws had been broken.
‘Withdraw and Repay’: Redfern Legal Centre
“If a COVID fine fails to state the specific offence, the fine is invalid,” Samantha Lee, senior solicitor at the Centre, said. “RLC considers that the judgment supports the conclusion that the remaining COVID fines are invalid and urges Revenue NSW to withdraw and repay the 29,000 remaining fines.”
Yet Commissioner of Fines Administration Scott Johnston, from Revenue NSW, told a Budget Estimates hearing that it would not be withdrawing any of the remaining fines, but will continue to “review and treat every matter on a case-by-case basis.”
However, Ms. Lee urged Mr. Johnston to “come to his senses.”
“The commissioner is refusing to honour a supreme court judgement and do the right thing and give people back their money and withdraw these fines that don’t meet the legal requirements,” she said. “We’re giving the commissioner time to come to his senses and make the right decision to withdraw these fines. If not, then watch this space.”
More than 33,000 COVID fines, worth millions of dollars, were cancelled after a NSW Supreme Court ruling in 2022 found that details of the offences were insufficient.
In that instance, Revenue NSW withdrew 33,121 fines, meaning roughly half of the 62,138 COVID-related infringement notices issued in the state during the pandemic were invalid. However, it emphasised that the decision to withdraw the fines did not mean the offences had not been committed.
*************************************************
13 March, 2024
New Zealand regulator ignored vaccine risks
The life of Ray Avery, a New Zealand-based scientist could come right out of a Hollywood screenplay. It is a rags to global influencer story. Known as ôSir Ray,ö he heads the Sir Ray Foundation. The author of two books including the bestselling autobiography ôRebel with Cause", chronicling his life from orphaned and homeless street-kid in England to actual Kiwi Knighthood.
The scientist, social activist, inventor and much more, Sir Ray founded Medicine Mondial, an independent agency focused on improving the lives of impoverished people around the world via distribution of high quality healthcare technology. In 2011, Sir Ray was honored as a Knight Grand Companion of the New Zealand Order of Merit by governor-general Sir Anand Satyanand.
Recently TrialSite featured Sir Rayĺs thoughts on the World Health Organization (WHO), and how it was never really possible to think the non-governmental organization funded by governments and wealthy donors could contain a global pandemic.
Now Sir Ray goes on the record, in the professional network LinkedIn to remind all that side effects linked to the COVID-19 vaccine are systematically ignored according to a response from the New Zealand Ministry of Healthĺs Medsafe (New Zealand Medicines and Medical Devices Safety Authority).
Reminding all about the role and importance of post marketing surveillance and ongoing monitoring of medicinal products once they reach the market after clinical trials. This includes the ongoing evaluation of vaccines for example, taken by individuals under a wide range of circumstances over an extended period of time.
According to Sir Ray, such surveillance ômust be conducted in perpetuum by the vaccine manufacturer to determine any long term adverse clinical effects due to the medicine and above all to validate the long-term safety and efficacy of the medicine.ö
It is an important topic given rare but real side effects such as the incident with 26-year-old male Rory Nairn who died after receiving the Pfizer mRNA-based BNT162b2 COVID-19 vaccine. This incident was reported in the Kiwi mainstream media such as 1 News.
In New Zealand, where Sir Ray resides, such tragic adverse event reports and records derive from The New Zealand Medsafe. The website states:
ôAnyone living in New Zealand who thinks they may have experienced an adverse reaction due to a medicine or vaccine can report it. You do not need to be a healthcare professional to report an adverse reaction.ö
According to Sir Ray, ôMedsafe collects and processes suspected adverse reaction reports and the physicians at the Centre for Adverse Reactions Monitoring (CARM) medically assess non-routine reports.ö
According to Medsafeĺs website on the topic of Post-marketing surveillance:
ôPost-marketing surveillance monitors the safety of medicines and medical devices in use. Products shown to be unsafe are removed from use, and prescribers are advised about new safety information for products. Post-marketing surveillance is achieved through activities such as:
monitoring adverse reactions to medicines used in New Zealand and monitoring the international literature and other information sources.
testing marketed medicines against product quality standards.
handling complaints and investigations; and
auditing and licensing medicine manufacturers.
Filing for OIA Request: Are they doing their job?
Under the Official Information Act (OIA) request, Sir Ray requested Medsafe to provide the number of adverse clinical events recorded for each Batch of Pfizer vaccine administered in NZ.
The New Zealand Governmentĺs official response:
ôMedsafe does not hold information on all recorded adverse events for medicines as these may be recorded in a patientĺs notes but not reported to CARM, and the batch may not be recorded. Therefore, this part of your request is refused under section 18(g)(i) of the Act, as the information requested is not held by the Ministry and there are no grounds for believing it is held by another agency subject to the Act.
What?
Sir Ray informs, ôSo, in plain English, no one in Medsafe or any medical related agency in NZ is monitoring and recording all serious adverse effects to individual Pfizer vaccine batches in NZ and many patient notes are not routinely reported to CARM ľ the Medsafe Adverse Drug reactions database.ö
Truly Troubling if True Reality
It is a troubling finding to say the least if fully verified. Sir Ray learns that since adverse clinical reactions in the original Pfizer trial were only followed up for two months, and as a consequence of that fact, post marketing surveillance of any serious adverse reactions to the vaccine becomes absolutely vital to demonstrate the long-term clinical safety and efficacy of the Pfizer vaccine, BNT162b2, developed in partnership with BioNTech from Germany.
Yet what Sir Ray has learned is that the New Zealand Government is failing to follow decades of obligation to ensure patient safety, not systematically monitoring recording all Kiwi-related serious adverse effects to individual Pfizer vaccine batches, plus the many patient notes are not routinely reported to CARM ľ the Medsafe Adverse Drug reactions database.
According to Sir Ray, ôIf you donĺt measure it, you donĺt know it is safe.ö
TrialSite has sent an email request to the Group Manager via multiple email contact addresses for clarification from the agencyĺs point of view.
A Message to New Zealand Ministry of Health
The health-related activist, philanthropist and entrepreneur has a serious message for the New Zealand government agencies responsible for this terrible gap in responsibility:
ôI urge Medsafe and the MOH to put in place an effective post marketing surveillance system to record ALL batch related adverse clinical effects due to the Pfizer Covid Vaccination.ö
Sir Rayĺs request in actuality represents a mandatory requirement for a pharmaceutical companies to gain and maintain ISO 13485 Certification to ensure the safety of the products that they manufacture, but they can only act of the feedback from Medsafe and New Zealandĺs Ministry of Health.
More on Medsafe
Medsafe is the New Zealand Medicines and Medical Devices Safety Authority. It is a business unit of the Ministry of Health and is the authority responsible for the regulation of therapeutic products in New Zealand.
With 60 operating staff and 2 offices according to the agencyĺs website, their mission is ôTo enhance the health of New Zealanders by regulating medicines and medical devices to maximise safety and benefit.ö
It would appear the agency falls short of their responsibility and their mission based on Sir Rayĺs investigational probing.
Who is running this agency?
Although the agency makes it very difficult to find what individuals actually fill the roles in the org chart below, TrialSite found that Christopher James runs Medsafe as Group Manager. A pediatric pharmacist by training, according to Mr. Jamesĺ own LinkedIn profile he has spent 17.5 years at the Ministry of Health New Zealand, serving as Group Manager for MedSafe Group Manager since 2015.
TrialSite reached out to Christopher James requesting that he respond and clarify on Sir Rayĺs allegations. Any response will contribute to an updated article.
*****************************************************
Does COVID-19 Vaccination Lower the Risk of Long-COVID?
The global healthcare system has faced numerous challenges due to the COVID-19 pandemic, with long COVID emerging as a major concernŚthe enduring, long-term effects of COVID-19 infection. Despite these challenges, Scientific American reported that the impact would have been more severe without vaccines. A consensus is emerging that individuals receiving higher doses of COVID-19 vaccines prior to infection experience a reduced risk of developing long COVID. This article will analyze this claim. TrialSite previously reported on the findings of a Nature article which purportedly provided evidence that COVID-19 vaccines reduce the risk of long-COVID in children and adolescents.
Long-COVID, also called post-COVID-19 conditions (PCC), is a condition in which individuals continue to experience a range of symptoms over an extended period after their initial COVID-19 infection. These can affect various parts of the body and can last for months and even years. Common symptoms of long COVID include fatigue, headache, shortness of breath, cough, chest pain, depression, and anxiety. According to an article by The Lancet, over 200 million people will develop the condition worldwide.
Vaccines may reduce the risk of long COVID
Studies highlighted by Scientific American shed light on the intricate interplay between vaccination and long COVID.
One was an observational cohort study published by JAMA in July 2022. The study included 2560 participants out of which 29% experienced COVID-19 and about 31% of those experienced long-COVID. Among unvaccinated individuals, the prevalence of long-COVID was 41.8%, while in vaccinated individuals, it was 30% with one dose, 17.4% with two doses, and 16% with three doses. Importantly limitations accompany this study, and the observational study cannot prove causation.
A systematic literature review published in Cambridge University Press in December 2022 concluded that receiving COVID-19 vaccination before or after getting an infection plays a major role in reducing post-COVID-19 conditions. This evaluation was based on ten studies with over 1.6M individuals. The vaccine efficacy in preventing long-COVID was 35.3% among individuals who received vaccination before infection and 27.4% among those who received vaccines after getting infected with SARS-CoV-2.
A meta-analysis published in the same journal in October 2023 was performed to investigate the long-term effects of vaccines on individuals. This analysis was based on 24 articles. The efficacy of vaccines against long-COVID was 36.9% among those individuals who received two doses before COVID-19 infection and 68.7% among those who received three doses before getting the infection. However, the analysis indicated that the vaccines did not protect from long-COVID symptoms for those who received vaccination after getting the infection. Ironically, some studies show that a combination of infection plus full vaccination (hybrid immunity) represents the strongest protection against future symptomatic COVID-19.
Another population-based cohort study was published in November 2023 by BMJ. This study was based on almost 600,000 individuals split into two approximately equal groups: one set that got vaccinated before getting an infection and the other that was unvaccinated at the time of infection. People who received one dose of the COVID-19 vaccine were 21% less likely to develop long-COVID symptoms. Having two and three doses of vaccine reduced the risk by 59% and 73% respectively. Based on the study results which are associated with its own limitations, the involved researchers suggest the more vaccine doses an individual gets, the more protection from long-COVID symptoms is observed.
Mixed effects of vaccines on long COVID symptoms
In addition to the peer-reviewed articles and meta-analyses looking at the incidence of long COVID, several studies have examined the effect of vaccines on the symptoms experienced by patients.
A study published in 2021 in the journal Vaccines was based on a survey of 396 patients who received at least one dose of vaccine within a year of becoming infected with COVID-19. Persistent symptoms at the time of vaccination were reported in 380 patients. After vaccination, 201 patients reported a change in their symptoms: 21.8% experienced improvement while 31% experienced worsening of symptoms, regardless of the vaccine type used.
Another study, published in the Journal of Medical Virology in 2022, investigated the changes in long COVID symptoms in COVID-19 patients after getting vaccinated. It reported a different conclusion. They evaluated the symptoms of 42 patients before and 14ľ21 days after their first dose of the vaccine. Results showed that the symptoms in 61.9% of patients remained unchanged, improved in 16.7%, and worsened in 21.4%. Importantly, the group that experienced worsening symptoms had higher antibody levels. The authors suggested that the vaccine might trigger an overly strong immune response that leads to the worsening of symptoms in long-COVID patients. They concluded that there is a need for careful monitoring to handle the additional concerns that may arise.
An observational study published by JIM in July 2023 aimed to examine the COVID-19 vaccine's potential to change the clinical presentation of long COVID. This study involved 477 individuals, of whom 245 were vaccinated. The results indicated that vaccinated people experienced fewer symptoms compared to unvaccinated individuals. The symptoms reduced with vaccination included abdominal pain, anosmia (loss of sense of smell), parosmia (distorted sense of smell), chest pain, dyspnea (shortness of breath), numbness, dizziness, and weakness.
https://www.trialsitenews.com/a/does-covid-19-vaccination-lower-the-risk-of-long-covid-59aeb9de
*************************************************12 March, 2024
According to Documents, Amazon ôFelt Pressuredö by White House to Censor COVID-19 Vaccine Books During Pandemic
In the midst of the Covid Pandemic, there was no question the Biden White House was deeply involved with Big Pharma to the point where a ôCovid Summitö was held in the presidentĺs residence. The event included all the major players who pushed the Covid vaccines, including Dr. Ashish Jah, who was the White House COVID-19 Response Coordinator, Dr. Anthony Fauci then director of the National Institute of Allergy and Infectious Diseases (NIAID), and Dr. Francis Collins the former head of the National Institutes of Health (NIH). Also in attendance were the representatives of pharmaceutical companies, including Moderna and Pfizer.
When Dr. Fauci addressed the summit, he pointed out that ôvaccines have saved over 2 million lives and prevented 17 million hospitalizations,ö and the emphasis on the summit was how vaccines will be developed and distributed. The summit extolled the virtues of the COVID-19 vaccine and was all in with Big Pharma, but how far did the Biden Administration go with their support of their Covid policy? Last month, it was revealed the White House may have ventured into censorship.
Email Trove
In early February, Congressman Jim Jordan, chairman of the House Judiciary Committee obtained internal emails from the White House which indicated that in early 2021, the Biden Administration pressured Amazon to censor books related to the COVID-19 vaccines. The White House was concerned the books available on the shopping site contained ôpropagandaö and ômisinformation.ö Andrew Slavitt, a former White House senior advisor on COVID-19, wrote in an email, ôWho can we talk to about the high levels of propaganda and misinformation and disinformation of [sic] Amazon? If you search for Ĺvaccinesĺ under books, I see what comes up,ö Slavitt wrote in a follow-up message the same day. ôI havenĺt looked beyond that but if thatĺs whatĺs on the surface, itĺs concerning.ö
Jordan has called the email trove ôThe Amazon Filesö and said, "Never-before-released internal emails subpoenaed by [House Republicans] reveal that the Biden White House pressured Amazon to censor books that expressed views the White House did not approve of." On his X account, Jordan added, ôWhy was the Biden White House so upset with Amazon? Because Amazon believed retailers are different than social media communities and provided their customers with access to a variety of viewpoints.ö ôFor the Biden Admin, letting Americans think for themselves was unacceptable.ö
Amazon Resisted, At First
In an email between Amazon executives, the White House idea of censorship was initially rebuffed. "We will not be doing a manual intervention today," one email said. "The team/PR feels very strongly that it is too visible and will further compound the Harry/Sally narrative (which is getting the Fox News treatment today apparently) and wonĺt fix the problem long-term ů because of customer behavior associates." The company sought not to attract attention regarding the governmentĺs concern but later met with officials because Amazon was ôfeeling pressure from the White Houseö and finally agreed to meet with administration officials. Later, Amazon instituted a "Do Not Promote" policy for books that were skeptical of vaccines.
TrialSite has experienced censorship during the COVID-19 pandemic firsthand, and this is why among other things the media company agreed to file a lawsuit along with presidential hopeful Robert Kennedy Jr against the Trusted News Initiative. See the link.
While TrialSite is an independent platform, censorship occurred when we shared information on social networks such as Facebook and YouTube. In all cases, TrialSite shared factual information that was censored, nonetheless. The situation has worsened. Now, on YouTube, if the World Health Organization hasnĺt blessed the topic, then YouTube will censor it, even if the news story is factual!
An example is the mass litigation against the HPV vaccine Gardasil manufactured by Merck. A TrialSite News story about the lawsuit was censored on YouTube, even though it was a 100% factual story. Why the censorship? Because the WHO hasnĺt addressed the Gardasil lawsuit topic, and that means it's labeled as ôMal-information!ö Anyone using their critical thinking skills can see itĺs a slippery slope toward fascism.
Back to the nationwide censorship during the pandemic, in a statement, the Biden Administration defended its actions, saying, "When confronted with a deadly pandemic, this Administration encouraged responsible actions to protect public health and safety. But our position has been clear and consistent: Although we believe tech companies and other private actors should take account of the effects their actions are having on the American people; they make independent choices about the information they promote."
But apparently, there are First Amendment questions. Jim Jordan is the chairperson of the House Judiciary Committee and Weaponization subcommittee and said he will hold investigations into how the White House dealt with Amazon.
And, this isnĺt the first time the Biden Administration has had issues regarding online content about the Covid Pandemic. In Missouri v. Biden three doctors, a news website, a healthcare activist, and two states, had posts and stories removed or downgraded by platforms. The plaintiffsĺ content touched on a host of divisive topics like the COVID-19 lab leak theory. They claim the government stifled their free speech, so they sued government officials for violations of their First Amendment rights. The case implicates the executive and other branches of the governmentĺs ability to impose policies and opinions, not through legislation but through verbal persuasion and ôjawboningö. The Supreme Court has already started hearing cases regarding the First Amendment and whether or not online content can be edited.
But the question here remains, regardless of motivation, did the Biden Administration cross the First Amendment line with their ôconcernö for the American public? Based on information coming out of discovery from trials such as Missouri and our own experience, weĺd have to say, unfortunately, our own government is, in some cases, spreading misinformation in a bid to disrupt the expression of accurate information. Thatĺs not to say that there is not a whole lot of garbage mis- and disinformation on X, formerly Twitter, for example. There is that as well. Itĺs ugly out there
*****************************************************
Court Finds Emergency Doctor Guilty of Misconduct for Questioning COVID Vaccine
Must not mention clinical experience?
A junior emergency room doctor in Western Australia has been found guilty of professional misconduct after giving a series of speeches and interviews critical of the governmentĺs response to the COVID-19 pandemic, and questioning the safety of the Pfizer vaccine.
Dr. Mitch Sambell, who has not practiced medicine since April 2023, has had his registration suspended for three months, and will be subject to a 12-month mentorship by another doctor.
Further, he has been ordered to pay a contribution of $2,500 toward the costs of the Medical Board of Australia, which sought review by the State Administrative Tribunal.
In a schedule of agreed facts, Dr. Sambell admitted to telling an interviewer that administering the vaccine to the wider populations was ôat best manslaughter, and at worst, like, outright murder.ö
He also described the director-general of the World Health Organisation as a ôcommunist.ö That interview was published on a video platform, Rumble, titled ôMedical Cover-Up in AustraliaŚAlbany Doctor Speaks Out.ö
ED was ĹFloodedĺ
When asked by the interviewer, ôCould you confidently say that people died in Australia from the vax jab?'ĺ
Dr Samball responded, ôOh, a 100 percent. Iĺve seen it. Iĺve seen it in ED. I saw so many people die in the hospital, so many people. Iĺve got people who are 40 that have heart failure after taking this vaccine ...ö
ôWhen it started getting rolled out I started seeing ED just got flooded; our hospital was at 117 percent pretty much all the time. And people say, ĹOh itĺs just a lack of staff, itĺs flu season,ĺ but it wasnĺt. We rolled out an experimental therapy to supposedly 95 percent of the population, and then our healthcare system couldnĺt cope.ö
He noted that the Australian Health Practitioner Regulation Agency has threatened disciplinary action against medical professionals who spoke out against the vaccine and said: ôThe truth always come out. And you can hide, and you can use your money, and you can manipulate things, but when people find out, youĺre in big trouble.ö
Dr. Samball repeated similar views at a public meeting in the Shire of Denmark in Western Australia in March 2022, saying, ôIf you are injected you can still acquire and spread the disease, so why are we allowing this issue to tear apart families, destroy businesses, and ultimately remove peopleĺs ability to choose a medical intervention without coercion, and therefore consent? ... Iĺm disgusted that the career I love has been used to destroy peopleĺs lives, and honestly Iĺm ashamed to be called a doctor.ö
The State Administrative Tribunal found these remarks ôlegitimised anti-vaccination sentiments and/or were contrary to accepted medical practice and/or were untrue or misleading,ö they were also ôdesigned to, or had the potential to, undermine public trust in the medical professionö and were inconsistent with the Code of Practice with which doctors are expected to abide.
In setting the penalty, the Tribunal noted that Dr. Samball had no previous disciplinary history, has made no public comment on the issue since 2022, and had ôshown insight and remorse.ö
The ruling has been criticised by newly appointed One Nation member and former Liberal Party MP, Craig Kelly, who said on social media it was ôMedical Fascism in Actionö and that ôAustralia is officially a medical fascist state.ö
https://www.theepochtimes.com/world/court-finds-emergency-doctor-guilty-of-misconduct-for-questioning-covid-vaccine-5604647
*************************************************
11 March, 2024
Colchicine saved lives among people with Acute COVID-19 -- a 32% Reduction in Mortality
Colchicine is normally used for the treatment and prevention of gout. It reduces inflammation which causes pain, swelling and other symptoms of gout. From the early days of the pandemic, some doctors have prescribed it to help with Covid
Umbrella reviews (sometimes called Ĺoverview of systematic reviewsĺ, Ĺoverviewĺ, Ĺreview of reviewsĺ, etc) are a new type of meta-evidence synthesis that has emerged in recent years to provide a birdĺs eye summary on a wide body of evidence on a determinate topic.5 6 Overall, umbrella reviews provide a single document that synthesizes an extensive body of information that could not be generated within a single publication for feasibility reasons and that direct readers to the current best evidence.
Danjuma et al performed an umbrella review of the meta-analyses summarizing the oral colchicine trials in acute COVID-19. Colchicine has been in the McCullough Protocol since 2020. The authors main findings were:
We included eighteen meta-analyses (n = 199,932 participants) in this umbrella review. Colchicine exposure was associated with an overall reduction of about 32% in the risk of mortality (odds ratio 0.68, confidence interval [CI] 0.58-0.78; I2 = 94%, p = 0.001). Further examination of pooled estimates of mortality outcomes by the quality effects model (corrected for the methodological quality and risk of bias of the constituent reviews) reported similar point estimates (OR 0.73; CI 0.59 to 0.91; I2 = 94%).
This is great news for those who were prescribed and took colchicine during the acute phase particularly early in the pandemic. The drug reduces inflammation in the chest an is commonly used now for myopericarditis, long-COVID, and other vaccine injury syndromes. Colchicine has a well-characterized safety profile.
********************************************
Hearing Delayed Again for BC Doctor Accused by College of COVID Vaccine Misinformation
WHITE ROCK, B.C.ŚThe B.C. regulatory body for doctors has again postponed a disciplinary hearing for a member accused of spreading ômisleading, incorrect, or inflammatoryö information in 2021 about COVID-19 vaccines and the governmentĺs pandemic response.
After having his earlier Feb. 13, 2023, hearing postponed, Dr. Charles Hoffe was rescheduled to appear on March 4ľ15 before the Discipline Committee of the College of Physicians and Surgeons of British Columbia.
However, on Feb. 16, nine businesses days before the hearing, the college submitted ôa 189-page application, referencing 43 case authorities and over 40 new documents, totaling in excess of a thousand pages,ö Dr. Hoffeĺs lawyer, Lee Turner, told The Epoch Times in an email.
Because he wouldnĺt have proper time to review the materials, Mr. Turner asked for an adjournment, and the college agreed.
The college has posted a notification of the adjournment on its website, but no new hearing date was provided.
Mr. Turner said he was subsequently informed that the college had applied for judicial noticeŚa rule surrounding evidence where, if some information is deemed commonly understood as fact, a judge can acknowledge it as such without requiring evidence to be provided and proven in court.
ĹEntirely Inappropriateĺ: BC Governmentĺs Proposed Changes to Oversight of Regulated Health Professions Draws Criticism
ôThe College alleges that the facts they seek judicial notice of are so notoriously known and well accepted that no reasonable person would dispute them,ö Mr. Turner wrote, adding, ôThe importance of such an application is obvious, as Dr. Hoffe disputes the facts alleged by the College.ö
Dr. Hoffe told The Epoch Times that if the request is granted, he would have no defence, as ôthe fact that theyĺre applying for judicial notice means they are trying to block me from being able to defend myself.ö
ôIf the disciplinary panel grants judicial notice, they are saying that all of the facts stated by the College are indisputable and thereĺs no debate,ö he said, and thus, effectively, ôthereĺs no trial, because I canĺt give any defence.ö
In an email to The Epoch Times, the college confirmed that it hasnĺt rescheduled the hearing and that it would not comment on the proceedings as they remain unsettled.
ĹWeĺre Not Scientistsĺ
Barry Bussey, a partner with law firm Bussey Ainsworth and president of the not-for-profit First Freedoms Foundation, said the rule of judicial notice has merit but its implementation should have a much higher standard than what heĺs seen in recent years, especially regarding information related to the COVID-19 pandemic.
ôIn Canada, we have yet to have a court that challenges the public health narrative that the government has been using,ö he said.
Mr. Bussey said whatĺs most frustrating for him is that tribunals or courts ôgive a path to who theyĺve determined are the expertsö concerning COVID.
ôWe give deference to the experts they have, and what the courts have often said under the COVID regime is ĹWeĺre not scientists. Weĺre not physicians. Weĺre not public health. We are judges, and therefore, who are we to question the experts?ĺ And yet, judges do it all the time.ö
One recent case is that of Dr. Mark Trozzi, an Ontario physician who had expressed concerns about the safety and effectiveness of COVID vaccination and in January had his medical licence revoked. This came after the Ontario Physicians and Surgeons Discipline Tribunal ruled in October 2023 that he ôengaged in disgraceful, dishonourable or unprofessional conductö and ôfailed to maintain the standard of practice of the profession.ö
In its ruling, the tribunal said it ôrelies on Health Canada regulatory approval of the COVID-19 vaccines as evidence of their safety and effectiveness,ö adding that ôjudicial notice should be taken of regulatory approval, and regulatory approval is a strong indicator of safety and effectiveness.ö
The tribunal also cited an Ontario Court of Appeal ruling in February 2023 on a different case related to COVID vaccination, which said, ôIt is not the subject of dispute among reasonable people that Health Canada has, in the area of safety and efficacy of medical treatment, Ĺspecial knowledge ů going beyond that of the trier of fact.ĺö
The Court of Appeal ruling attributed the ôspecial knowledgeö quotation to an even earlier ruling by the Supreme Court of Canada, from 1993, and added: ôRequiring that opinion to be tendered viva voce in every case via live, human experts would beŚ especially in family courtŚunnecessarily burdensome.ö
ĹA Serious Issueĺ
However, in another COVID-19 vaccination case decided by the Ontario Superior Court of Justice in August 2022, the judge said he was not comfortable accepting government information and opinion on COVID vaccines as safe and effective for children, and therefore, judicial notice could not be used.
As part of his decision, Justice Corkery outlined how judicial notice regarding COVID vaccine safety had been taken in several court cases to date but refused in others.
ôThe issue before the court in taking judicial notice of scientific facts is not assessing whether the science is Ĺfake science,ĺ but whether scientific facts that would normally require expert opinion to be admitted, may be judicially noticed without proof,ö he wrote.
ôThe science relating to COVID-19 is developing. The Ĺfactsĺ are changing,ö he added, saying, ôI am not prepared to take judicial notice of any government information with respect to COVID-19 or the COVID-19 vaccines.ö
Balancing whether a court or tribunal takes judicial notice amid a contested set of facts demands an even higher level of scrutiny, particularly when someoneĺs career is at stake, says Marty Moore, litigation director with Charter Advocates Canada.
ôI would expect that judicial notice needs to be applied robustly in either sense, especially when youĺre prosecuting a doctor,ö Mr. Moore told The Epoch Times.
ôThe potential consequence of removing a licenceŚa serious issueŚneeds to be dealt with requiring fairness to the individual. And if youĺre going to say you can only challenge the facts that we allow you to challenge, thatĺs obviously not a fair process.ö
ĹDecisions Based Upon Ideology or Partisanshipĺ
Leighton Grey, senior partner with Grey Wowk Spencer LLP, says he believes judicial notice has been overused in cases related to vaccines and government measures applied to the public.
In emails to The Epoch Times, he described how he feels judicial notice has been misused and how Dr. Hoffeĺs hearing may be challenging for the doctor.
ôJudicial notice is where the court regards as proven a fact that could not possibly be disputed,ö Mr. Grey wrote.
ôCourts did this throughout the pandemic in relation to the government and mass media COVID narratives such as Ĺvaccines are safe and effective.ĺ I am speaking of how courts repeatedly accepted the government narrative about COVID-19 and Ĺvaccines,ĺ and that they continue to do so. Rather than being a Constitutional check upon government overreach, they became a branch of the administrative state.ö
Noting that Dr. Hoffe has to first defend himself at an administrative tribunal, Mr. Grey said winning the battle against judicial notice is only his first hurdle.
ôThe other problem with administrative tribunals is that they are populated by persons appointed by government for their politics, so that they will render decisions based upon ideology or partisanship,ö Mr. Grey said.
ôIt may very well be that Dr. Hoffe is dealing with just such a situation,ö he added.
Dr. Hoffe says he began noticing patients experiencing severe adverse events from the Moderna COVID-19 vaccine injections at his practice in the rural town of Lytton, B.C., in early 2021, shortly after the vaccine rollout. He reported these reactions to other medical personnel in his community, but was quickly rebuked by Interior Health, the provincial health authority that oversees his area, and asked not to direct his concerns to his colleagues.
After Interior Health ignored his repeated requests to address his concerns, he went public with an open letter to B.C. Provincial Health Officer Bonnie Henry in April 2021. Interior Health responded by removing his hospital privileges.
Then in February 2022, the College of Physicians and Surgeons of B.C. issued a citation against him.
The college alleged that he ôcontravened standards imposed under the Health Professions Act, including but not limited to the Canadian Medical Associationĺs Code of Ethics and Professionalism by publishing statements on social media and other digital platforms that were misleading, incorrect or inflammatory about vaccinations, treatments, and public measures relating to COVID-19.ö
*************************************************
10 March, 2024
Veterans Affairs Kept COVID-19 Vaccine Mandate in Place Without Evidence
7 March, 2024
Excess Deaths Since 2022 Primarily in Vaccinated, Official Data Suggest
Excess deaths since 2022 were primarily in the vaccinated, official data suggest, fuelling fears that the Covid vaccines may be playing a significant role in the high excess deaths in recent years.
Data from the Office for National Statistics show that the proportion of total deaths in England among unvaccinated people dropped sharply in early 2022, even as excess deaths soared. The proportion then remained low throughout the following two years, indicating that the additional deaths during this period were concentrated in the vaccinated.
Is this why the authorities continue to resist releasing the full data on deaths by vaccination status? A cross-party group of 21 MPs and peers are the latest to write to request the data be released. Are the authorities refusing because they know the data show excess deaths predominantly in the vaccinated?
The striking effect was seen in every age group. The charts showing these results can be seen below (find the data here, table 5). The blue lines show the total deaths by month in the age group (left-hand axis) while the red lines show the proportion of deaths in the unvaccinated in the age group (right-hand axis; unvaccinated here means receiving no doses). The most striking feature on each chart is the steep drop in the red line in early 2022, which denotes a sharp and sustained drop in the proportion of deaths in the unvaccinated and a corresponding rise in the proportion in the vaccinated.
Note this is not because more people got vaccinated at that time, as the number getting their first dose in these age groups was almost zero by this point (see chart below, taken from here, data here). People getting their first dose may affect the trends seen in 2021, particularly in the first part of the year, though the over-60s were largely done with first doses by June 2021.
Itĺs worth pointing out that by using only death data they avoid the problems with the ONS population estimates highlighted by Professor Norman Fenton and others that have tended to exaggerate the death rate in the unvaccinated.
Note that the red lines during 2022 and 2023 are mostly flat, particularly for those in their 60s, 70s and 80s, even during many of the peaks in total deaths. This is particularly noticeable during winter 2022-23, where despite a large peak in deaths the red lines stay largely flat. This suggests that vaccine efficacy against death, at least from the Omicron variants, is very low, since if the virus was disproportionately killing the unvaccinated (i.e., the vaccines were protecting the vaccinated) the proportion of deaths in the unvaccinated should spike during waves. That it usually does not suggests low vaccine efficacy.
These charts include no comparison with death rates before the vaccination period so donĺt allow us to say very much about the pre-Omicron period as there is little to compare it to. However, there are notable spikes in the red lines for those over 70 during the Delta wave of late 2021. On first sight this would seem to indicate vaccine efficacy against the Delta variant during that winter. Things may not be so straightforward, however. Notice that the other largish spike for those over 80 is in summer 2022. Importantly, this was not associated with a Covid wave; instead it was associated with a heatwave ľ that was when the heat dome was sitting over Europe causing record temperatures. This is significant because the vaccine obviously does not protect against heatwaves. This means the reason for the summer 2022 spike is not vaccine efficacy. What is it then?
It seems likely it is related to the Ĺhealthy vaccinee effectĺ i.e., the fact that people who take vaccines tend to be people with better background health outcomes than those who donĺt take vaccines. A number of studies indicate that vaccinated people have a background death rate around half that of unvaccinated people (this is a background death rate not related to vaccine efficacy or safety).
The poorer background health of the unvaccinated group means that any general cause of death that disproportionately affects the frail or those with comorbidities, such as a virus epidemic or a heatwave, will naturally, other things being equal, disproportionately affect the unvaccinated group, for reasons unrelated to the vaccine. This would explain the summer 2022 spike in the red lines and it may also explain some or much of the spike during the Delta wave as well. Assuming this is right, it makes the lack of spikes during other waves, such as winter 2022-23, even more striking, as one would normally expect the unvaccinated group to be disproportionately affected by a virus wave or a winter, yet instead the lines remain flat. These flat red lines during waves of deaths are therefore also potentially indicative of a concentration of excess deaths in the vaccinated.
The headline finding from these charts is the striking concentration of excess deaths in the vaccinated after early 2022, just as Omicron appeared. This worrying observation may be why the authorities are keeping the full data, which would confirm or rule out such a finding, firmly under wraps.
********************************************************
Lockdowns Are a ôFailed Experimentö, Welsh First Minister Tells Covid Inquiry
The BBC reports that Walesĺs First Minister Mark Drakeford has told the Covid Inquiry that local Covid lockdowns were a ôfailed experimentö.
He could have said it was a failed policy or intervention, but Drakeford chose to say lockdowns were an ôexperimentö.
An experiment is a scientific procedure undertaken to make a discovery and test a hypothesis.
However, at the time, lockdowns were a policy enforced by law.
Mark Drakeford announced in May 2020 that the maximum fine for repeated breaches of the lockdown rules in Wales rose from ú120 to ú1,920. Up to June 8th, 2,282 Fixed Penalty Notices were issued for ľ as it seems now ľ failing to participate in an experiment. People in Wales were twice as likely as English to be fined for breaking lockdown rules. Some experiment.
We are at a loss to explain how the people who set the laws can do so based on experiments. As for experiments, where was the consent procedure, where was the control group and where was the evaluation?
The Welsh Governmentĺs Chief Scientific Adviser for Health, Rob Orford, read from the evidence Drakeford provided to the inquiry that ôin hindsight perhaps they werenĺt the best ideaö.
Yet again, we learned that policy wasnĺt based on any evidence. ôIĺm not sure where the origin of the idea around local interventions came from, whether that was the U.K. Government or Welsh Government.ö
We utterly reject the ôhindsightö argument, which Sir John Edmunds also used as an excuse for some of his most extreme advice.
We reject it because we pointed out the obvious on April 8th 2020: you cannot affect the circulation of an endemic respiratory virus with any of the interventions known to us, including vaccines, which were not on the table then.
We pointed out that wrecking society and the economy to chase an evidence fallacy was the stuff of nightmares. We and the rest of society have paid a heavy price for this temerity.
Policy must be based on expertise and evidence. If there is no evidence, you either generate it or sit on your hands as the precautionary principle suggests, until such time as the costs and benefits of alternative actions are clear.
*************************************************
Airline Fined $250,000 For Standing Down Worker Concerned With COVID-19
Australian national carrier Qantas has been fined $250,000 after standing down a workerŚwho was an elected health and safety representativeŚafter he raised concerns about the risk of COVID-19 to staff cleaning aircraft that had arrived from ChinaŚan action the judge described as ôshameful.ö
Lift truck driver Theo Seremetidis was employed by subsidiary Qantas Ground Services (QGS) at Sydney International Airport, and was sidelined in early 2020, before which he had worked for Qantas for nearly seven years as a ground crew fleet member.
Last year, NSW District Court Judge David Russell found the airline engaged in discriminatory conduct, ruling that Mr. Seremetidis was unfairly cut off from other staff who were seeking his help.
ôThe conduct against Mr Seremetidis was quite shameful,ö the judge said. ôEven when he was stood down and under investigation, QGS attempted to manufacture additional reasons for its actions.ö
Last week Qantas agreed to pay Mr. Seremetidis $21,000 for economic and non-economic loss.
On March 6, Judge Russell ordered that QGS be convicted and fined $250,000, finding that the companyĺs conduct involved significant culpability and was deliberate, rather than inadvertent and that QGS had ôdeliberately ignoredö the consultation and other provisions of the Work Health and Safety Act. He said there was a ôgross power imbalanceö between Mr. Seremetidis and senior managers at QGS.
Mr. Seremetidis was ômost conscientiousö in carrying out his role as a health and safety representative, the judge found, staying up-to-date with official announcements about the pandemic and even doing research on his day off.
Judge Russell found QGS saw Mr. Seremetidisĺs directions to cease unsafe work as a ôthreatö to the conduct of the business, in particular to its ability to clean and service aircraft and get them back in the air, and pointed out that the role of health and safety representatives was ôvitalö to the protection of workers and the running of any business.
During the hearing last year, Qantas said it had taken the action because Mr. Seremetidis had been ôcreating anxiety amongst the workforce.ö
It was revealed the airline had told concerned workers that the risk of them contracting COVID-19 from their work was ônegligible,ö and they could not ôbe reasonably concerned about contracting the virus.ö
Prosecutor Matthew Moir said Qantas gave priority to its commercial interests over the health and safety of its workers. But Qantas lawyer Bruce Hodgkinson argued the airline had been doing its best to deal with the fast-unfolding pandemic.
Qantas Apologises
A Qantas spokesperson said the airline accepted the penalties. ôWe agreed to compensation for Theo Seremetidis and the court has today made orders for that compensation to be paid,ö the spokesperson said.
ôWe acknowledged in court the impact that this incident had on Mr. Seremetidis and apologised to him. Safety has always been our number one priority and we continue to encourage our employees to report all safety-related matters.ö
*************************************************
6 March, 2024
Large Real World-Evidence Study Finds COVID-19 Vax + Paxlovid Benefit Against Hospitalization
Nirmatrelvir-ritonavir (Paxlovid) developed by Pfizer, is an antiviral medication that is indicated for individuals with mild-to-moderate COVID-19 who are at risk of progression to severe COVID-19. While initially studied on unvaccinated persons, a growing number of observational investigations provide evidence of the potential for significant protection by Paxlovid against hospitalization among vaccinated individuals at elevated risk for severe COVID-19.
Not a lot of data avails scientists seeking to assess the risk reduction from antivirals together with vaccination. Here, the study team led by researchers from the U.S. Center for Disease Control and Prevention (CDC) as well as the U.S. marketĺs leading electronic health record (EHR) vendor Epic to estimate the stepwise benefit of monovalent vaccination and Paxlovid against COVID-19 hospitalization in the United States. Overall, the findings complement previous research indicating Paxlovid affords additional protection in high-risk individuals, even if vaccinated.
The findings here, according to the joint CDC and Epic team, complement previous research pointing to the protective overlay afforded by Paxlovid in high-risk individuals, even if vaccinated.
This line of research had not yet examined the protection of treatment and vaccination combined. Treatment with Paxlovid without vaccination does not reduce risk of hospitalization to levels seen in treated individuals with three or more vaccinations.
While the burden and impact of COVID-19 in future respiratory seasons are uncertain, the authors of this study suggest the combination of vaccination and oral antiviral treatment for eligible patients remains an important tool against COVID-19 hospitalization and death. The CDC Advisory Committee on Immunization Practices recently recommended the 2023-2024 (monovalent, XBB-containing) COVID-19 vaccines in persons ? 6 months of age. The CDC-led study paper suggests clinicians should consider treatment with Paxlovid among all adults who are at high-risk of severe COVID-19 disease, including vaccinated persons.
Important Caveat
Importantly, this study was limited to adults infected with COVID-19 during the period April and August 2022, and may not be applicable in the current landscape of population hybrid immunity and SARS-CoV-2 strain evolution. The authors acknowledge that more updated estimates over time are necessary to better understand the impact of vaccination and antiviral treatment. The risk-benefit analyses for COVID-19 vaccination have likely changed. Plus, the medical establishment to date has yet to accept the dozens of peer reviewed manuscripts showing risk with the mRNA induced spike protein, capable of distribution in tissue and organs throughout the body, albeit in rare to relatively rare cases.
There are risks associated with COVID-19 vaccination that are not openly talked about in mainstream media, or even to this day in the trade press; but they are discussed in TrialSite, an independent, objective unbiased (as humanly possible) media platform tracking the world of biomedical research. Additionally, the SARS-CoV-2 pathogen has become milder during the Omicron stage, with a case fatality rate similar to influenza. Of course, the risk increases with age as well as co-morbidities and immunocompromised status.
The Study
The CDC and Epic research team conducted the retrospective analysis of patient records in Cosmos, a real world-evidence dataset that, at the time of this study, included EHR information from >160 million individual users of U.S health systems covered by Epic. Inclusion criteria and definitions were described previously in a prior study of real-world effectiveness of nirmatrelvir-ritonavir in this population. Non-pregnant adults were eligible for inclusion if aged ?50 years or if aged ?18 years with an underlying health condition associated with progression to severe COVID-19 disease documented in their medical record. All included patients had a COVID-19 diagnosis (defined as a diagnostic code or positive SARS-CoV-2 test result) associated with an outpatient encounter during April 1ľAugust 31, 2022, indicating mild-to-moderate COVID-19.
The investigational team considered patients to have received nirmatrelvir-ritonavir (Paxlovid) if verified it was prescribed during the five days after their COVID-19 diagnosis. Vaccination status was categorized on the date of COVID19 diagnosis using data available in the Cosmos system. As reported in the journal Clinical Infectious Diseases, vaccination categories included 1) unvaccinated if no COVID-19 vaccine had been received; 2) 2 mRNA vaccine-dose recipients if ?14 days had elapsed since receipt of the second dose and no subsequent doses had been received or <7 days receipt of third dose; 3) ?3 mRNA vaccine-dose recipients if ?7 days had elapsed since receipt of the third dose; and 4) other vaccine recipient if any Janssen (Johnson & Johnson) vaccine, other vaccine, or only 1 mRNA vaccine dose had been received any time before COVID19 diagnosis.
The primary outcome was COVID-19 hospitalization within 30 days after diagnosis. A COVID-19 hospitalization was defined as having a COVID-19 specific diagnosis associated with the admission.
The group estimated protection against hospitalization by the Paxlovid combination combined with COVID19 mRNA vaccination based on statistics generated from Cox regression. Presenting adjusted hazard ratios (aHR) for hospitalization adjusting for age group, sex, race and ethnicity, social vulnerability index of the address of residence, number of underlying health conditions, region of residence, and previous infection defined as having a COVID-19 diagnosis code or positive SARS-CoV-2 test result (nucleic acid amplification or antigen) >90 days prior to the included COVID-19 diagnosis.
The reference group comprised unvaccinated individuals who had not received Paxlovid.
Results
Among the unvaccinated, 35,826/141,931 (20.2%) received Paxlovid compared to 42,355/157011 (27.0%) of patients who received 2 mRNA doses, and 130,778/330,448 (33.0%) of those who had received 3 or more mRNA vaccine doses.
During AprilľSeptember 2022, 5,296 of 731,349 patients (0.72%) with COVID-19 were hospitalized within 30 days after their initial diagnosis.
Hospitalization Rates
After receipt of nirmatrelvir-ritonavir and 3 or more mRNA vaccine doses, there were an estimated 16.9 fewer hospitalizations per 100,000 person-days compared to those who were unvaccinated and untreated.
According to the group of authors:
ôCompared with patients who were unvaccinated and had not received a COVID-19 treatment, the rate of COVID-19 hospitalization was lower among both those who were vaccinated but did not receive nirmatrelvir-ritonavir (two mRNA doses, aHR 0.74, 95%CI: 0.67ľ0.80; three or more mRNA doses, aHR 0.51, 95%CI: 0.47ľ0.55) and those who were unvaccinated but after receipt of nirmatrelvir-ritonavir (0.47, 95%CI: 0.40ľ0.55).
After receipt of both treatment and vaccination, the hospitalization rate was reduced further (two mRNA doses and nirmatrelvir-ritonavir aHR 0.33, 95%CI: 0.29ľ0.39) with the lowest rate of COVID-19 hospitalization among those after receiving three or more mRNA vaccine doses and nirmatrelvir-ritonavir (aHR 0.22, 95%CI: 0.19ľ 0.24).ö
***********************************************
How low can Covid catastrophists go?
Whoĺd have guessed that there would be two startling revelations about the great Covid over-reach in the space of about a week, upholding claims previously dismissed as conspiracy theories and misinformation?
First came a peer-reviewed scientific study which linked Covid vaccines to a range of serious health disorders. It was soon followed by the Queensland Supreme Court ruling that vaccine mandates imposed on police and ambulance workers in the state were unlawful.
Both provided a welcome dose of reality after the worst days of lockdowns and vaccine roll-outs when we were bombarded with the message that the jabs were Ĺsafe and effectiveĺ. Years later, we know for certain that they do not prevent contraction or transmission of the virus and thereĺs an acknowledged chance they could cause serious harm and even death.
Some of us have been aware of this for a long time, but vaccine promoters, including Big Pharma and government bureaucrats, insist that the risk is Ĺvery lowĺ, the acknowledged disorders are Ĺrareĺ, and that vaccines provide the best means of protection against Covid.
But how low is Ĺvery lowĺ and how Ĺrareĺ is rare? Letĺs look at the latest findings from the largest vaccine safety study to date conducted by the Global Vaccine Data Network. A research division of the World Health Organisation, it reportedly looked at 99 million vaccinated individuals across six continents.
The study confirmed connections between Covid vaccines produced by Pfizer, Moderna, and AstraZeneca to several serious but Ĺrare conditionsĺ.
According to a report in Forbes:
While the side effects are serious, the chance of experiencing them is low. Some highlighted increases include a 6.1-fold increase in myocarditis from the second dose of the Moderna mRNA vaccine. Cases of pericarditis had a 6.9-fold increase as a result of the third dose of the AstraZeneca vaccine. There is a 2.5-times greater risk of developing Guillain-BarrÚ syndrome from the AstraZeneca vaccine along with a 3.2-times greater risk of developing blood clots from the same vaccine. There is a 3.8-times greater risk of getting acute disseminated encephalomyelitis from the Moderna vaccine, and a 2.2-fold increase in the AstraZeneca vaccine.
When choosing to get vaccinated, it is important to weigh the benefits and risks of the vaccine. Information like this makes it easier to make the right choiceů
Well thanks, but my wife and I made that choice a few years ago and we remain very glad we did, given there are some still trying to pedal the message that a six to seven times chance of contracting a serious heart condition is Ĺlowĺ.
Iĺm reminded of the old Chubby Checker hit Limbo Rock, ĹHow low can you goĺ? Much lower than that, if you want to convince people the vaccines are safe ľ let alone effective.
My own long-term scepticism possibly has links back to my first job after leaving high school many moons ago, when I undertook a pharmacy apprenticeship in a very busy regional pharmacy.
Maybe it didnĺt help when I was questioned by a detective when a patient died after taking a sleeping mixture I had dispensed, even though I was later cleared after forensic tests showed the medicine contained the correct level of ingredients and the poor bloke had swallowed an overdose. But possibly the last straw had something to do with a drug I had dispensed many times to pregnant young women suffering morning sickness. Finally, the authorities woke up to the fact that the Ĺcureĺ ľ thalidomide ľ was causing horrific birth defects. Sound familiar?
Fast forward to February 2021, when the novel Covid vaccines were rolled out in Australia after being developed and approved in record time without long-term human trials. Manufacturers were granted immunity from liability for subsequent mishaps despite some of these companies having records of huge fines for past problems.
There were also experts, including highly qualified epidemiologists, sounding warning bells, particularly in Europe and America. Some adverse events might only become apparent months or even years after the jabs were administered, but that was dismissed as ratbag conspiracy theory, disinformation, and misinformation.
Well not any more, and hopefully the Queensland Supreme court ruling that some of these vaccine mandates were unlawful will lead to justifiable and wide-ranging compensations.
As Rowan Dean wrote in The Spectator Australia, ĹThe news, of course, is to be welcomed. It is the first crack in the dam wall and will hopefully be followed by significant class actions and further court casesůĺ
Here, here! And letĺs hope that the issue does not become bogged down in appeals courts by a government with a guilty conscience and deep pockets.
Finally, my short-lived dispensing career was never a waste of time and it actually saved one of our young sonĺs lives when a pharmacist dispensed the wrong medication which I recognised as a potent heart drug that could have stopped his from beating!
Again, thatĺs another story.
https://www.spectator.com.au/2024/03/how-low-can-covid-catastrophists-go/
*************************************************5 March, 2024
COVID-19 Vaccines Can Affect Menstrual Cycle, Researchers Find
Researchers confirmed that COVID-19 vaccines are linked to changes in the menstrual cycle, according to a study published in March.
Published in the Obstetrics & Gynecology journal on March 1, Oregon Health & Science University researchers found that women who received a COVID-19 shot in the first half of their menstrual cycle are more likely to receive cycle length changes than those who received the vaccine in the second half.
Those researchers used data from 20,000 users of a birth control app that was approved by the U.S. Food and Drug Administration (FDA) to determine what effects the vaccine has on the cycle. Most of the women whose data was analyzed were under the age of 35, while 28 percent were from North America, 33 percent were from Europe, and another 32 percent were from the United Kingdom, they said.
Some were vaccinated and some were not. For those who were vaccinated, 63 percent received an mRNA vaccine, the paper said.
ôIndividuals vaccinated in the follicular phase experienced an average 1-day longer adjusted cycle length with a first or second dose of COVID-19 vaccine compared with their pre-vaccination average,ö the authors of the paper said, referring to women who got a dose of the vaccine during the first half of their cycle.
Those who got the vaccine in the second half or those who were not vaccinated experienced no changes, they found.
The authors added that there is now ôa body of evidence demonstrating that the ... vaccine is associated with temporary menstrual cycle disturbances at the population level,ö adding that ôthe underlying mechanism for a vaccine-related cycle length disturbance is still under investigation.ö
ôThe leading hypothesis is that these disturbances are due to the immune response that vaccines are designed to produce,ö the study said, adding that ôthe immune and reproductive systems interact closely with one another.ö Cytokines, which are small proteins that control the immune systemĺs activity and are produced ôas an early event in the vaccine response,ö can impact that process, they added.
Little research has been conducted in the past on how vaccinesŚwhether for COVID-19 or othersŚcould influence the menstrual cycle, the studyĺs authors further noted.
Responding to the studyĺs findings, Dr. Alison Edelman, the lead author of the paper with the Oregon university, said that ôwe do know the immune and reproductive systems interact closely with one another,ö adding that with vaccinations, ôit is certainly plausible that individuals may see temporary changes in their menstrual cycle due to the immune response.ö
Their findings also suggested that there may be changes in the length of the cycle, although they appear to be short-lived. But they added that women who notice significant changes should contact a healthcare provider.
And earlier in 2022, another set of researchers wrote that for women who received one of the COVID-19 vaccines, around 42 percent of respondents said they experienced increased menstrual bleeding. A majority of those who werenĺt menstruating reported breakthrough bleeding after getting the shot, including two-thirds of women who were post-menopausal and slightly less than two-thirds of women who were using hormone treatments.
Most respondents received an mRNA vaccine made by either Moderna or Pfizer. But some also received Novavax, Johnson & Johnson, and AstraZeneca shots, according to the paper.
ôWe focused our analysis on those who regularly menstruate and those who do not currently menstruate but have in the past. The latter group included postmenopausal individuals and those on hormonal therapies that suppress menstruation, for whom bleeding is especially surprising,ö Kathryn Clancy, a professor of anthropology at the University of Illinois Urbana-Champaign, said in a statement about the studyĺs findings at the time.
And it is not the first time that the same Oregon Health & Science University researchers found COVID-19 vaccines are associated with a change in the cycle. In 2022, they found that the change was pegged at under one day, and no change in menses length was detected.
While the study did not find vaccination associated with changes in menses length, ôquestions remain about other possible changes in menstrual cycles, such as menstrual symptoms, unscheduled bleeding, and changes in the quality and quantity of menstrual bleeding,ö they wrote.
Pfizer Officialĺs Concerns
About a year ago, a Pfizer employee was seen in an undercover video telling a reporter with Project Veritas that he was concerned about the mRNA shotĺs possible side-effects relating to menstrual cycles.
ôThere is something irregular about the menstrual cycles. So people will have to investigate that down the line because that is a little concerning,ö the Pfizer official said in the video, adding that it ôshouldnĺt be interferingö with the cycles.
ôI hope we donĺt discover something really bad down the line,ö he later added.
****************************************************
COVID-19 Shot Hesitancy Driven by Knowledge of Adverse Events
People who did not comply with COVID-19 vaccine requirements were hesitant because they knew someone who had experienced a health problem after getting the injection, according to recent research.
ôKnowing someone who experienced a health problem following COVID-19 injection reduced the likelihood of injection, the International Journal of Vaccine Theory, Practice, and Research reported.
Such people ôwere more likely to oppose injection mandates and passports.
Conversely, ôknowing someone who had health problems following the COVID-19 illness increased the likelihood of injection,ö the journal said.
Among those who were aware of at least one individual who experienced COVID-19 injection adverse events, they said they knew about 57 deaths following vaccination.
ôThe health issues reported ranged from serious problems such as cardiac arrests and other heart-related problems, blood clots and other circulatory problems, to neurological issues, as well as milder effects such as feeling sick, headache, fever, etc.ö
The study, published on Feb. 16, investigated the factors that made people support or protest COVID-19 vaccine mandates and passports. Researchers collected information from an online survey completed by 2,840 individuals in December 2021.
It found that 22 percent of the respondents knew at least one person who experienced a health issue after getting vaccinated.
The authors cited other studies on vaccine hesitancy in the context of influenza to point out that ôvaccination status [in these studies] is influenced by beliefs regarding vaccine safety, effectiveness in infection prevention, and the gravity of the illness that might be prevented.ö
They cited a survey published by Rasmussen Reports in March last year which found that ônearly as many Americans believe someone close to them died from side effects of the COVID-19 vaccine as died from the disease itself.ö
This survey combined with the results of the present study ôaffirms that opposition to COVID-19 injection mandates and passports has increased over time,ö the researchers wrote.
Moreover, the findings of the study suggest that policymakers may find it difficult to ôengender a consensusö when it comes to pushing for vaccine mandates and passports, the researchers stated.
The study found that having COVID-19 illness was not associated with preferences for injection mandates. However, those who were injected were found to be ômuch less likely to oppose injection mandates than are those that did not receive the injection.ö
Race was a ôstrong predictorö of injection mandates, with minority populations like African Americans, Hispanics, and Asians being ôless inclinedö to oppose such regulations than Caucasians.
ôPolitical identity is also important: Compared to Democrats, those who self-identify as Republicans are more likely to oppose mandates. Those who identify as Independent also tend to oppose injection mandates.ö
One of the authors of the study is Mark Skidmore, a professor and Morris Chair in State and Local Government Finance and Policy at Michigan State University (MSU). He has previously published research in several journals like Economic Inquiry, Economics Letters, and the Journal of Urban Economics. The second author, Fernanda Alfaro, is a Ph.D. student at MSU.
Regarding funding and conflicts of interest, researchers said they received funds from an individual donor.
Safety Concerns and Vaccine Hesitancy
In a recent post at the International Center for Law and Economics, health economist Roger Bate points out that the COVID-19 vaccines ôwere not as effective as originally claimed, and were effectively forced onto many people in order for them to work, attend school, or travel.ö
ôThere is early evidence that these and other factors may currently be contributing to heightened vaccine hesitancy, with potentially serious consequences for public health.ö
A July 2022 analysis published in BMJ Global Health also raised similar concerns. It argued that mandatory COVID-19 vaccination policies were ôscientifically questionableö and were more likely to result in harm than good.
ôRestricting peopleĺs access to work, education, public transport, and social life based on COVID-19 vaccination status impinges on human rights, promotes stigma and social polarisation, and adversely affects health and well-being,ö it said.
The restrictive COVID-19 policies ômay lead to a widening of health and economic inequalities, detrimental long-term impacts on trust in government and scientific institutions, and reduce the uptake of future public health measures, including COVID-19 vaccines as well as routine immunizations.ö
In an interview with Fox News last year, Dr. Robert Redfield, former head of the Centers for Disease Control and Prevention (CDC), said that federal officials pushed a ôfalse perceptionö that the COVID-19 vaccines provided ôcompleteö immunization.
ôThere was such an attempt to not let anybody get any hint that maybe vaccines werenĺt foolproof, which, of course, we now know they have significant limitations,ö he stated.
ôI always said ů my position was just tell the American public the truth: There are side effects to vaccines. Tell them the truth, and donĺt try to package it.ö
Commenting on the Feb. 16 study, cardiologist Peter A. McCullough said in a Substack post that vaccine hesitancy would be higher in 2024 ôas more injuries, disabilities, and deaths have been reported as a result of the novel genetic productsö since the 2021 survey.
ôWhen it comes to COVID-19 vaccination, hesitancy is a good thing demonstrating the population is concerned about consumer product safety of the mRNA and adenoviral DNA technology,ö he wrote. Dr. McCullough also criticized the American Medical Associationĺs (AMA) view on vaccine hesitancy.
The AMA website has this statement: ôWhile the AMA is a strong advocate for the effectiveness and safety of vaccines, we recognize that some members of the public may have historical, cultural, or religious reasons to distrust the vaccination process.ö
The AMAĺs views on the factors driving vaccine hesitancy are inapplicable, Dr. McCullough said. ôAttempts to overcome vaccine hesitancy are likely to be harmful.ö
Some experts have also raised concerns about vaccine hesitancy triggered during COVID-19 extending to other vaccines as well.
*************************************************
4 March, 2024
CDC drops 5-day isolation guidance for COVID-19 cases
The Centers for Disease Prevention and Control on Friday rolled back its longstanding five-day isolation guidance for people who come down with COVID-19.
Under the updated guidelines, the CDC says those infected with the coronavirus can return to work or the public just one full day after their fever subsides.
“Today’s announcement reflects the progress we have made in protecting against severe illness from COVID-19,” agency Director Dr. Mandy Cohen said in a statement.
“However, we still must use the commonsense solutions we know work to protect ourselves and others from serious illness from respiratory viruses—this includes vaccination, treatment, and staying home when we get sick.”
The guidelines for isolation have not been updated since Dec. 2021, when CDC had shortened the recommended isolation time for Americans with asymptomatic cases to five days from the previous guidance of 10 days.
The announcement follows reports last month that the policy change was in the works due to a decrease in infections.
The US has seen an overall decline in COVID-19 cases — 17,300 people were hospitalized and 510 people died from the virus during the week of Feb. 17, the most recent CDC data available.
The updated guidelines, however, do not affect workers at nursing homes and other health care facilities. Medical personnel should follow recommendations to stay home at least seven days after symptoms first appear, and that they test negative within two days of returning to work, according to the CDC.
While the guidelines have been significantly scaled back, health officials are still urging sick persons to take extra precautions in the first five days following an infection.
Those with COVID-19 are encouraged to stay home until 24 hours after a fever, stay up to date with vaccinations, wearing a mask and social distancing — all of which reflects guidelines similar to other highly contagious viruses.
“While every respiratory virus does not act the same, adopting a unified approach to limiting disease spread makes recommendations easier to follow and thus more likely to be adopted and does not rely on individuals to test for illness, a practice that data indicates is uneven,” the CDC said in the announcement.
https://nypost.com/2024/03/01/us-news/cdc-drops-five-day-isolation-rules-for-covid-19-infections/
************************************************Covid pandemic could have been avoided and contained to Wuhan, professor claims
The Covid pandemic could have been avoided and contained to Wuhan, a professor has claimed in a damning book that lifts the lid on Chinese blunders that allowed the virus to spread across the globe and kill millions of people.
'Wuhan: How the Covid-19 Outbreak in China Spiraled Out of Control', by leading author Professor Dali Yang was published on Friday and explores the pandemic in forensic detail.
Prof Yang draws a devastating conclusion that the pandemic, which started with the first known patients in the eastern Chinese city in late December 2019, was not inevitable.
The book explores key events that came before a lockdown was imposed on Wuhan, including how a mass banquet was held on January 18 that saw more than 100,000 people come together despite health officials knowing the virus was spreading.
Prof Yang offers a deep analysis of who knew what and when about the virus, but barely touches on the origins of Covid-19, The Telegraph reports.
It instead looks at the individual heroism seen during the pandemic as well as the flawed decision-making and lack of clarity as officials tried to deal with a mysterious 'pneumonia of unknown etiology'.
Prof Yang concludes that the global pandemic, which led to the deaths of an estimated 13.3 to 16.6million people worldwide, could have been prevented.
'I do think there was a meaningful chance that the pandemic could have been avoided,' Prof Yang, a political scientist at the University of Chicago, told The Telegraph.
The professor believes that Chinese health authorities were dealt a 'remarkably strong hand of cards' in the early days of the virus breaking out.
'China is a country with significant capabilities, which could have advanced the knowledge and response more rapidly at the end of December 2019,' he added.
But he says any advantage was destroyed by a authoritarian political system that was not prepared for the emergency.
The pandemic dates back to when several of Wuhan's doctors at some of China's best hospitals discovered that a 'pneumonia of unknown etiology' in the city was showing sign of 'human-to-human' transmission.
Experts had feared that the virus was linked to the SARS coronavirus that plagued East Asia between 2002 and 2004. On doctor told the local Centre for Disease Control (CDC): 'It's a disease we've never encountered before, it's also a family [cluster of] infections. Something is definitely wrong!'
Coronavirus was confirmed by Vision Medicals, a lab based in Guangzhou, who tested 'Patient A' - a 65-year-old man with severe pneumonia and 'multiple scattered patchy faint opacities in both lungs'.
'Due to the sensitivity of the diagnostic results', the lab only confirmed the positive test result for a SARS-like coronavirus to the hospital over the phone and not in writing.
Doctors found it was 81 per cent similar to the first SARS coronavirus outbreak. And screenshots that appeared online showed the virus was instantly recognised as something that 'should be treated in the same class as the plague' in order to contain it.
Despite growing evidence pointing towards a possible pandemic, the local CDC was slow in its response.
Gao Fu, the director general of the national CDC, only head about the Wuhan outbreak via social media on December 30.
And while he acted swiftly with emergency responses, the next few weeks were marred by mistakes, censorship and political interests which failed to stop the virus spreading rampantly.
'The first week in January became a pivotal turning point for handling the outbreak. Just the wrong kind,' the book states. 'The failure to act before January 20 was monumental.'
One of the biggest mistakes was failing to respond to several cases in Wuhan that were not linked to the Huanan Seafood Market - the location of the first clusters.
Prof Yang suggests that when the market was therefore closed, people believed the virus was under control and the virus was able to spread amid a false sense of security.
Other factors that contributed to working against containing the virus was China's political tradition of suppressing information to maintain social stability.
'Clearly many [doctors] are heroes but, if you read between the lines, they also operated within constraints,' Prof Yang said.
'It's clearly not a black and white picture but shades of grey. Some of the most heroic doctors happened to be also ones who might not have spoken up like they could have. It's a very complicated picture.'
Doctors who did speak out were reprimanded by police and infections among hospital staff were covered up .
Even as Wuhan moved closer towards a lockdown, high-profile events such as Chinese New Year celebrations were still showcased to try and prove everything was under control.
It was Taiwan’s Dr Chuang Yin-ching who said the outbreak was much worse than feared on January 13 2020. When he returned, Taiwan issued a travel alert for Wuhan and tightened border controls.
But back in Wuhan, the severity of the virus continued to be downplayed and it was left to Dr Zhong Nanshan, 83, a trusted veteran of the first SARS epidemic, to warn that Covid was 'certainly transmissible from human to human'.
He confirmed that cases were being seen in Beijing, Guangdong, Shanghai, and Zhejiang and even abroad in Japan, South Korea and Thailand. At this point, China was put on alert and citizens were advised to wear face masks.
However, New Year celebrations still took place in the Wuhan and Hubei province, with residents invited to apply for 200,000 free passes to visit landmark sites. Local media praised performers for continuing despite being sick.
By the time Wuhan was sealed off from the rest of the world on January 23, some 500,000 people had left the country for the holidays.
*************************************************
Lockdowns may be GOOD for you
Strange findings
Lockdowns during the Covid pandemic led to two 'fascinating' changes in babies bodies that may have protected them against disease and allergies, a study has found.
Researchers from University College Cork in Ireland found that children born while the world was locked down during Covid had an altered gut microbiome - the ecosystem of 'good' and 'bad' bacteria in the gut that aid in digestion, destroys harmful bacteria and helps control the immune system.
The biome was found to be more beneficial in the infants.
Researchers believe this led 'Covid babies' to have lower than expected rates of allergic conditions, such as food allergies, compared to pre-pandemic babies, the scientists found.
They also required fewer antibiotics to treat illnesses.
Researchers analyzed fecal samples from 351 Irish babies born in the first three months of the pandemic, between March and May 2020, and compared them to samples from babies born before the pandemic.
Online questionnaires were used to collect information on diet, home environment and health to account for variables.
Stool samples were collected at six, 12 and 24 months and allergy testing was performed at 12 and 24 months.
The Covid newborns were found to have more of the beneficial microbes gained from their mother after birth, which could act as a defense against allergic diseases.
If individuals have a disrupted gut microbiome, this may lead to the development of food allergies.
Babies born in the pandemic had lower allergy rates: About five percent of the Covid babies had developed a food allergy at age one, compared to 22.8 percent in the pre-Covid babies.
Researchers said that mothers had passed on the beneficial microbes to their babies while pregnant, and they gained additional ones from the environment after they were born.
The study also found that babies born during lockdowns had fewer infections because they were not exposed to germs and bacteria.
This meant they needed fewer antibiotics - which kill good bacteria - leading to a better microbiome.
The lockdown babies were also breastfed for longer, which provided additional benefits.
Of the Covid babies, only 17 percent of infants required an antibiotic by one year of age.
In the pre-pandemic cohort, meanwhile, 80 percent of babies had taken antibiotics by 12 months.
This was 'fascinating outcome,' joint senior author Liam O'Mahony, professor of immunology at the University College Cork, said, and 'correlated with higher levels of beneficial bacteria such as bifidobacteria.'
Professor Jonathan Hourihane, consultant pediatrician at Children's Health Ireland Temple Street and joint senior author of the study, said: 'This study offers a new perspective on the impact of social isolation in early life on the gut microbiome.
'Notably, the lower allergy rates among newborns during the lockdown could highlight the impact of lifestyle and environmental factors, such as frequent antibiotic use, on the rise of allergic diseases.'
The researchers hope to re-examine the children when they are five years old to see if there are any long-term impacts of the early changes in gut microbiome.
The study was published in the journal Allergy.
*************************************************
3 March, 2024
CDC Tracking BA.2.87.1, New Omicron Subvariant With Potential to Evade Immunity
Experts detected a strain of SARS-CoV-2 with more than 30 changes in its spike protein compared with Omicron subvariant XBB.1.5, the US Centers for Disease Control and Prevention (CDC) announced. The newer Omicron subvariant, known as BA.2.87.1, has infected at least 9 people in South Africa since September 2023. No cases have been reported in the US or outside South Africa, the CDC noted in its update.
The large number of changes in spike proteins raises the possibility that the new strain could escape the immunity people have acquired from vaccines or infection. Still, the relatively few cases suggest the variant is not highly transmissible right now.
Although the CDC is carefully monitoring the new strain, the agency expects that current vaccines and treatments will continue to be effective.
https://jamanetwork.com/journals/jama/fullarticle/2815864
***************************************************Scientist claims Ĺsmoking gunĺ evidence COVID-19 intentionally created by researchers in Chinese lab
COVID-19 may have been created in a Chinese lab, a British professor told the UN Wednesday, with another expert claiming that evidence of the likelihood has reached ôthe level of a smoking gun.ö
Richard H. Ebright, a molecular biologist at Rutgers University, was quoted saying in a new Wall Street Journal article that the virus that killed millions around the world may actually have been manmade in Chinaĺs Wuhan Institute of Virology.
He cited evidence found in a 2018 document from the lab that talked of making such a virus.
ô[The document] elevates the evidence provided by the genome sequence from the level of noteworthy to the level of a smoking gun,ö Ebright said in the piece by former New York Times editor Nicholas Wade.
The papers from the lab cited by Ebright contained drafts and notes regarding a grant proposal called Project DEFUSE, which sought to test engineering bat coronaviruses in a way that would make them more easily transmissible to humans.
The proposal was ultimately rejected and denied funding by the US Defense Advanced Research Projects Agency, but Wade suggested that their work could have been carried out by researchers in Wuhan who had secured Chinese government funding.
ôViruses made according to the DEFUSE protocol could have been available by the time Covid-19 broke out, sometime between August and November 2019,ö wrote Wade, a former science editor of the New York Times.
ôThis would account for the otherwise unexplained timing of the pandemic along with its place of origin.ö
Along with the research notes, Wade claimed the specific genetic structure of the coronavirus that allowed it to infect humans served as another strong indication of ôthe virusĺs laboratory birth.ö
ôWhereas most viruses require repeated tries to switch from an animal host to people, SARS-CoV-2 infected humans out of the box, as if it had been preadapted while growing in the humanized mice called for in the DEFUSE protocol,ö Wade wrote.
While scientists continue to debate whether the coronavirus pandemic was a natural occurrence or manmade, Ebright believed there was credibility that the work proposed by the now-controversial EcoHealth Alliance led to the development COVID-19.
Following the release of the 2018 documents Ś which were published by US Right to Know through a Freedom of Information Act request Ś Ebright said there was clearer evidence that the virus was manufactured in a lab, the Daily Telegraph reported.
The 2018 documents contained drafts and notes regarding Project DEFUSE and how to synthesize bat coronaviruses to make them more transmissible.
The researchers proposed introducing ôappropriate human-specific cleavage sitesö to the spike proteins of SARS-related viruses in the lab, the same method several biologists have said could have been used to synthesize the coronavirus that led to the pandemic.
According to the documents, the researchers had planned to conduct a portion of the research at the Wuhan lab where they noted that safety conditions were not up to US standards, to the point where they claimed American scientists would ôlikely freak out.ö
While COVID-19ĺs origins remain a mystery, Dr. Filippa Lentzos, an associate professor of science and international security at Kingĺs College London, said the world needed to acknowledge that the possibility exists that the virus was synthesized.
Speaking before the UN in New York on Wednesday, Lentzos presented the work of the Independent Task Force on Research with Pandemic Risks, which calls on scientists the world over to follow stricter regulations lest another worldwide breakout occur, the Telegraph reports.
ôWe have to acknowledge the fact that the pandemic could have started from some research-related incident,ö Lentzos said.
ôAre we going to find that out? In my view, I think itĺs very unlikely that we will. We need to do better in the future,ö she added. ôWe are going to see more ambiguous events.ö
https://nypost.com/2024/02/29/world-news/scientists-may-have-started-the-covid-pandemic-article/
**********************************************************Angry nurses rally at Gold Coast University Hospital, demand jobs back
A vindictive bureaucracy at work. They don't like admitting that they were wrong
Dozens of placard-waving nurses and other healthcare workers took part in the rally outside Gold Coast University Hospital on Saturday.
It followed fury this week after The Courier-Mail revealed leaked Queensland Health emails telling a veteran nurse that ôwe are unable to re-employ any staff who were officially terminatedö for refusing the jab.
Queensland Health boss Michael Walsh said the edict was incorrect and wrote to all hospital and health services in the state on Friday telling them there was no directive not to reinstate sacked workers.
Health Minister Shannon Fentiman this week repeatedly denied there were any barriers to hundreds of workers who refused to comply with the vaccination mandate from returning to work.
But nurses protesting on the Gold Coast said they were still struggling to get their jobs back.
They included 23-year veteran intensive care nurse Michelle Williams, who said she tried to reapply at the major hospital she was sacked from in 2021 but was told there were no vacancies - only to see a job ad for a position.
ôItĺs frustrating, itĺs really frustrating,ö she said. ôPatients are suffering and theyĺve got very junior staff looking after them. ôThereĺs so many of us with so much experience and our experience is just going to waste.ö
Ms Williams said Ms Fentiman needed to ôstop lying to usö.
ôWe want to come back to work, weĺve done nothing wrong except not follow this one (vaccine) direction,ö she said. ôWeĺre not criminals. Weĺre people who love our jobs, we love looking after patients and we just want to help people. ôWe just want to come back to work and do what we love doing, and thatĺs helping people get better.ö
Ella Leach, secretary of the Nurses Professional Association of Queensland, said Ms Fentiman had not responded to an invitation to attend or at least endorse the rally.
Ms Leach said the minister had been sent the names and experience of 350 sacked health care workers who wanted to return and ôShannon should be reaching out to them directlyö instead of making them reapply.
ôThereĺs just zero excuse ů we want her to take some actual action,ö she said.
ôThese people were born to be nurses and health professionals - they want to work. It doesnĺt make them happy hearing that the systemĺs crumbling, it makes them desperately angry and upset. ôAll they want to do is work.ö
Ms Leach was herself sacked from Queensland Childrenĺs Hospital for refusing the vaccine - in January this year, four months after the mandate was lifted, and despite being seven monthsĺ pregnant. She launched unfair dismissal action against Queensland Health.
Ms Leach said many sacked healthcare workers who had reapplied for jobs with Queensland Health were still being rejected because of their ôdisciplinary action historyö in refusing the vaccine.
ôThese people have decades of experience and they are desperately needed,ö she said.
Ms Leach said 6000 nurses were predicted to retire in 2024 but Queensland Health was hiring nurses from interstate or overseas, with incentives of up to $70,000.
*************************************************
Also see my other blogs. Main ones below:
http://edwatch.blogspot.com (EDUCATION WATCH)
http://antigreen.blogspot.com (GREENIE WATCH)
http://pcwatch.blogspot.com (POLITICAL CORRECTNESS WATCH)
http://australian-politics.blogspot.com (AUSTRALIAN POLITICS)
http://snorphty.blogspot.com (TONGUE-TIED)
https://immigwatch.blogspot.com (IMMIGRATION WATCH)
https://awesternheart.blogspot.com (THE PSYCHOLOGIST)
http://jonjayray.com/blogall.html More blogs
*********************************************************